
Injuries to the lower leg are quite common with compartment syndrome being the hardest to diagnosis, and one of the only non-traumatic injuries in the leg that may require surgery. Many cases of Shin Splints are actually tibial or fibular stress fractures which may be quite self limiting (time is a great cure for these). Severe calf cramping (with the meaning of “severe” different from patient to patient and doctor to doctor can be a warning sign of a venous blood clot (not to be ignored). I will focus here on the common injuries/pain syndromes that a podiatrist will treat in the leg on a daily basis called shin splints, but could be stress fractures, muscular strains, acute tears of the muscles ( “Tennis Leg”), and the less common DVTs and compartment syndromes that one needs to be on the lookout for.
Shin Splints
Shin Splints: What are they? What is the basic treatment?
Shin Splints literally means pain somewhere between below the knee joint and above the ankle joint. There are a lot of structures that can produce pain in that area, so the treatments range from simple to complex. Mostly, shin splints is an overuse of one group of muscles/tendons that start (originate) in the leg, and end up (insert) into part of the foot. Each one of these muscle/tendon has various functions around various joints. It can be one of these muscle functions that has been forced to work in an overuse fashion that produces pain. Podiatrists, physical therapists, orthopedists, chiropractors, and physiatrists (rehab specialists) tend to be the most qualified to recognize the exact muscle/tendon involved when treatment is stalling.
Shin splints is so common, and normally responds so well to basic treatment, that most clinicians do not get too involved in its complexities. The basic treatment of shin splints involves:
- Reduce activity to pain free levels for at least one week.
- Ice the involved area for 30 minutes 3x/day.
- Change your athletic shoes if they may be worn down.
- Minimize your speed workouts and hill workouts.
- Consider if levels of Calcium and Vitamin D may be low.
- Attempt 3 to 4 days/week alternative exercises as long as it is pain free (i.e. cycling, elliptical, walking, swimming, court sports, etc.)
- Stretch the achilles tendon 2 positional (knee straight and knee bent) for 1 minute each 3x/day.
- Experiment with an ankle brace or ankle taping if it is painful to walk.
- Wear tie-on supportive athletic shoes full time while the shin is healing (although you may experiment with clogs as an alternative).
- Attempt pain free muscle strengthening of the muscle group involved.
As your symptoms get better, gradually increase your activity back to normal levels (normally 15% increase per week if you were still able to exercise, and 10% per week if you had to shut it all down). A walk/run program may be an appropriate starting point.
Now, let us review the anatomy of Shin Splints. The 4 basic types of shin splints are Medial (most common), Anterior (2nd), Lateral (3rd), and Posterior (4th).
Medial shin splints involve a group of muscles (with most commonly associated muscle function) including the posterior tibial (controls over pronation), flexor hallucis longus (stabilizes the big toe), and the flexor digitorum longus (stabilizes toes 2 to 5). Photo below shows where medial shin splints occur. Since over pronation, bunions (unstable big toes), and hammertoes (unstable lesser toes) are all common problems, this type of shin splint is the most common. More specific treatments of these problems include various methods in controlling pronation, stablizing the big toe area or stablizing the lesser toes.These include toe separators/spreaders, shoe inserts with Morton’s extensions, big toe spica taping to stabilize the big toe area, and toe crests, toe taping, reverse Morton’s extensions all to stabilize the lesser 4 toes.
Medial shin splints involve a group of muscles (with most commonly associated muscle function) including the posterior tibial (controls over pronation), flexor hallucis longus (stabilizes the big toe), and the flexor digitorum longus (stabilizes toes 2 to 5). Photo below shows where medial shin splints occur. Since over pronation, bunions (unstable big toes), and hammertoes (unstable lesser toes) are all common problems, this type of shin splint is the most common. More specific treatments of these problems include various methods in controlling pronation, stablizing the big toe area or stablizing the lesser toes.These include toe separators/spreaders, shoe inserts with Morton’s extensions, big toe spica taping to stabilize the big toe area, and toe crests, toe taping, reverse Morton’s extensions all to stabilize the lesser 4 toes.

Many patients purchase shoes too wide in the toe box leading to marked instability, especially when they have bunions. Too much room with resultant sliding around is just as bad on bunions and hammertoes as having too little room with resultant crowding. To help stabilize, the patient will grip with the toes, possibly producing medial shin splints. Even good fitting shoes initially can begin to loosen up as it breaks down. Try power lacing to help gain stability. Runners can also get medial shin pain commonly from tibial stress fractures. The 2 most common places for tibial stress fractures are distal medial (just above the ankle) and posterior (presently as calf pain or medial shin splints).

The 2nd most common form of shin splints is anterior shin splints (see photo above). The muscles (functions) involved all help to control foot slap after heel strike, and then to help lift the foot off of the ground at toe off. Overuse situations can easily occur with hill running and increases in the speed of workouts. It is the most commonest form of shin splints in the first month of cross country season, so common that most coaches ignore since the muscles due tend to get strong. The muscle/tendons involved are the anterior tibial (controls over pronation and stabilizes the first metatarsal), extensor hallucis longus (stabilizes big toe and lifts toe up at toe off), extensor digitorum longus (stabilizes lesser toes and lifts these toes up at toe off), and the peroneus tertius (stabilizes the outside of the foot including the cuboid , 4th metatarsal and 5th metatarsal). When the peroneus tertius is involved there can be a problem with over supination just like lateral shin splints.
This muscle group is normally the weakest of the 4 groups and has to constantly pull against the more powerful Achilles tendon. As the calf/Achilles gets too tight/too strong with vigorous exercise, it is hard for the anterior group to keep up. These muscles will strain under the added stress of working against the tight Achilles. Hopefully, when someone has anterior tibial shin splints, treatment should be directed towards:
• Stretching of the calf
• Decreasing hills/speed for awhile
• Stabilizing pronation (medial support) or stabilizing supination (lateral/cuboid area support)
• Stabilizing any digit appearing unstable (with toe separators, taping, toe crests, etc.)

The 3rd most common form of shin splints is lateral shin splints (see photo above). The muscle/tendons (functions) involved are the peroneus longus (stabilizes the lateral ankle against excessive supination and stabilizes the cuboid and the first metatarsal), and the peroneus brevis (stabilizes the lateral ankle against supination and stabilizes the cuboid and fifth metatarsal). So together they stabilize the lateral ankle, and both sides of the midfoot area. Ankle braces, ankle proprioceptive exercises (see post below on flat footed balancing), power lacing, and stable shoes if you pronate or supinate too much can all be part of the treatment.

The 4th common form of shin splints is posterior shin splints (see photo above). The upper 2/3 of the calf is considered a shin splint if the pain is deep. This can be a stress fracture on the posterior aspect of the tibia (very common in runners) and often misdiagnosed as calf muscle strain. It may also be a strain of the soleus muscle (deep part of the calf) where it originates on the tibia. The gastrocnemius (or gastroc) is the bigger, more superficial, muscle of the calf. The soleus muscle starts deep to the gastroc and becomes the other ½ of the Achilles tendon below. Therefore, the soleus functions to lift the heel. It also attempts to slow down pronation at heel contact, so over pronators may strain the muscle. It is harder to strengthen the soleus then the gastroc, so weaknesses may develop and muscle strains can occur with relatively minor overuse situations.
In general, soleus strengthening is done with the knee bent 45 to 90 degrees and the ankle is then plantarflexed with resistance (pointed downward like a ballerina on her pointe shoes). Treatment of this type of shin splints must initially rule out a tibial stress fracture which requires other treatments and concerns. Once tibial stress fractures are ruled out by x ray or bone scan typically, functional changes include decreasing ankle plantarflexion (extension) and stabilizing pronation. Also, avoiding activities that produce a negative heel effect where your heel is unsupported and drops below the plane of the forefoot, like getting off your seat in cycling. A slight biomechanical change in activities to minimize heel lift (ie. walking more flatfooted even when going up hills, or lowering the seat on your bike) can greatly speed up treatment.
This time of the year (September and October especially) is made for Shin Splints. Cross Country season is starting and all high school and some college coaches are drowning in Shin Pain. Most of the time the athlete's pain is related to the bone and muscles not being used to the activity and overuse occurs. A shin splint technically is when the muscle pulls so hard on the bone that the lining of the bone (called the periosteum) is pulled away from the bone causing bleeding between the bone and bone covering. This normally is improved with time, icing, some stretching, and activity modifications.
However, when the bone is weaker (poor base of running, low Vit D or Calcium, low estrogen, abnormal bone structure) than the muscle, the bone may actually be the weakest link in the chain and break. This break in the bone normally remains a stress hairline fracture not detectable by normal xrays. Only in rare cases does the bone break all the way through into a complete fracture. The complete fractures are easy to diagnosis, due to the intense pain. A hairline stress fracture, also called a fatigue fracture of the bone, can at times be run on for weeks and even months. Top athletes, with apparently high pain thresholds, have presented to our office with 3 to 5 stress fractures and still running with so-called "shin splint pain". More reading below on the Weakest Link in the Chain concept.
So, when shin splints are not improving with the simple measures of relative rest, ice, shin sleeves, cross training, shoe changes, stretching and strengthening, etc, I advocate the use of a bone scan. It is positive within several days of a stress fracture, and is less expensive than an MRI. In our hospital, for the same price you get both legs for comparison, where MRIs are now being charged for only one side at a time and small areas at a time.
Christina, a freshman X-Country runner in high school presented with significant pain right greater than left tibias. Definitely she could not run through this pain. Bone Scans below documented a stress fracture only on the left side. The right tibia had generalized increase uptake of the dye which we call pre-tibial stress fracture or tibial stress reaction. Stress reactions can hurt just as much as a stress fracture, although heal quicker.
 |
On this front view of the tibias, see the intense dye uptake in the middle of the left tibia. Since Christina is fourteen, she is still growing so her growth plates near the knees and ankles are still very active.
|
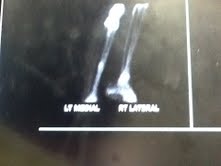 |
Here is a side view of both tibias with the left again showing the spot where the tibia broke.
|
This is also a good example of why MRIs probably would have mislead us in Christina's case. Christina had more pain on her right side. Due to the expense of MRIs, and the fact that each side has a separate cost, I probably would have only done the right side. I would not have found the fracture, and probably allowed her to run sooner. We never will know. So consider getting a limited bone scan instead of an MRI when shin splints are not improving. Thank you Christina for being a good model, but sorry your shins hurt.
No comments:
Post a Comment
Thank you very much for leaving a comment. Due to my time restraints, some comments may not be answered.I will answer questions that I feel will help the community as a whole.. I can only answer medical questions in a general form. No specific answers can be given. Please consult a podiatrist, therapist, orthopedist, or sports medicine physician in your area for specific questions.