Treatment for Short Leg Syndrome
Limb Dominance with Short Leg Syndrome
The lean to the left in this runner who just happens to be my wife Pat can be caused by a short leg.
When you watch someone walk, there may be a slight lean to one side which is very consistent. This is caused by many problems, including scoliosis and short leg syndrome. When evaluating for a possible short leg, look for this lean known as "limb dominance". Pat is demonstrating left side dominance. If you have received lifts for a short leg, the lifts should eliminate all or most of this lean. Never use lifts if the perscriber does not watch you walk and/or run with and without them documenting their success. Never use lifts if the lean is made worse by the lifts. If your symptoms seem to be getting worse with lift therapy, stop using lifts for a week to verify that the symptoms are being caused by the lifts. When they work, it is wonderful and life changing. When they do not work, search for a reason.
When you are walking along, do you ever notice you always drift to one side or the other? Do people who walk with you comment that you always bump them if they walk on your right or left side? Do they sometimes joke that you won't pass a sobriety test even when sober? If you walk with hard soled shoes on a hard surface, do you hear one side landing harder (greater sound)? These can all be clues of a short leg. With a short leg, you may lean to the long or the short side, but most adults lean to their long side.
In my practice I treat short leg for many reasons, but the most referrals I get are for hip and low back pain patients. Iliotibial band syndrome is also commonly caused by a short leg. When a patient is always injuring the same side, even though different areas, think short leg syndrome. Lifts to correct for the uneven hips and pelvis can allow the muscles to function equally on both sides of the body easing stress points and allowing muscle imbalances to correct. If you have any clues you may have a short leg, and you are having pain, perhaps lift therapy to correct for the short leg may be helpful for you.
Short Leg: Heel Lifts vs Full Length Lifts
The 9 common biomechanical categories used in the treatment of injuries are:
Short Leg Syndrome (discussed here)
Poor Shock Absorption
Excessive Pronation
Excessive Supination
Tight Muscles
Weak Muscles
Miscellaneous Gait Abnormalities (ie Drop Foot, Polio, etc)
Forefoot Abnormalities
Combinations of the Above
The heel lift is the main method used in treatment of short legs and their problems. But, heel lifts are inherently unstable, and easy for patients to compensate for by simply bending the knee on that side. Once you bend the knee on the side you are trying to lift, you have lost the correction. Heel lifts, therefore, can make the foot/ankle more unstable by lifting your heel up in the shoe more, and they can make the knee more unstable by producing greater knee bend/flexion.
Doctors are always placing the lift onto an orthotic device. This is not advisable. First of all, it makes it hard to decide what symptoms are related to the lift, and what symptoms are related to the orthotic device, if pain increases with orthotic devices. Secondly, because of the instability mentioned above, the heel lift may negate the added stability produced by the orthotic device.
Golden Rule of Foot: Keep orthotic devices and lifts for short legs totally separate.
Thirdly, most of the lifts I have seen attached to orthotic devices are very hard for durability, but poor for impact shock absorption.
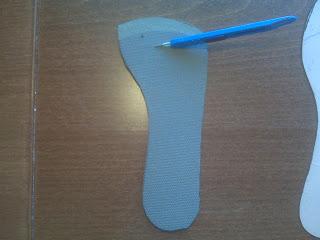
Full length lifts in the treatment of short leg syndrome are much more stable and produce better symptom relief. Full length lifts need to lift the heel and forefoot (metatarsal area) equally, then taper at the toes. This full length lift above, designed around a shoe insert template for W9 (women's size 9), is actually cut off at the toes to give room in the toe box area. Imagine all of the athletes who run up on the ball of their feet, but need a lift for their short leg, how could a heel lift do anything positive for their biomechanics and symptoms? At least 50% of the time most athletes are on the ball of the foot while exercising, so a full length lift seems ideal for the athletic population.

Now athletes on the other hand would love the lift to be only under the heel for convenience and shoe fit, but it is so much better to have it full length. Compromises are made all the time for lifts between ¼” and ½” (in even roomy athletic shoes or dress shoes with removable foot ends), typically the full lift needed is placed under the heel with ½ of the lift at the ball of the foot.
If you use full length lifts, make sure you make cuts into the material by the ball of the foot to help with smooth push off. This is especially true as you get up over 1/4 inch in lift. Material under the ball of the foot can make it hard to move through, so cutting to increase bend, along with beveling and thinning slightly can all help.
You can also see that the front edge of the full length lift is bevelled or skived to make a smoother transition forward. When I am using full length lifts, I always try to get feedback from the athletes on how easy it is to move through their foot.
In podiatry talk, I am trying to avoid Sagittal Plane Blockade.
You can see the cuts do not go through the sides to help with its durability, but they do go completely through from top to bottom.
Not really demonstrated well, but these cuts do improve the bend of the foot making it easier to move gently through to the toes. Many shoe repair stores have material to make a shoe lift.
Short Leg Treatment: Shoe Lifts
Most patients have a short leg, either structurally or functionally, or a combination of both. A structural short leg is true length difference of the bones, where a functional short leg may be caused by many factors including one arch lower than the other side. As long as one arch collapses more than the other side, the short leg syndrome exists.

Most people have one foot longer than the other, but the long foot may or may not be on the long leg. Remember you are taught to buy shoes always for the longer side (longer foot). If you wear out one shoe more than the other, either by observing the heel of the outersole or the footbed within the shoe, you can tell that one leg may be shorter. Orthopedists normally do not recommend treatment for leg length differences unless over 1/2". Podiatrists have observed that as little as a 1/16” to 1/8" difference in leg lengths can cause symptoms. By treating these small differences, and having patients report positive outcomes, leg length discrepancies are a vital part of care.
Treatment of leg length discrepancies is with various types of lifts under the short leg. The photo above shows a shoe with a full length external or outersole lift of 3/8". Due to the swelling in his foot, this patient could not tolerate any lifts within the shoe. Full length lifts, whether within the shoe or on the outer sole, are normally so much more stable than just heel lifts as previously discussed.
Most athletic shoes can accommodate up to 3/8" lifts. All patients should have a trial of lift therapy with shoe inserts with positive results before external shoe lifts are utilized. Most shoe repair shops can put on external lifts, but there may be one in your area that specializes. Ask around for referrals from local orthopedic or podiatry offices. The external lift must be tapered at the toes, and somewhat flexible at the ball of the foot, to allow the patient to walk smoothly from heel to toe. Any external shoe lift pushes the foot away from the bottom of the foot, so mechanically until we adapt to it, you must be careful walking on stairs (foot strike is earlier).
Golden Rule of Foot with lift therapy: Start Low, Go Slow. Normally, if the difference is 3/8" total, 1/8" lift is given for 2 weeks, then another 1/8" lift for 2 more weeks, then finally the full 3/8". As you go up in lift therapy, blame any new symptoms on the added lift, take out the additional lift until the new symptoms subside, then try again. Some patients are stuck for one reason or another at one level of lift. Their bodies will reject the higher amounts. There seems to be more stress on the body when the exact same lift is placed on the outsole, or as a midsole lift, as was originally used as an insert. It probably weighs slightly more, or affects the motion around heel strike more. To lessen this change, which may cause symptoms itself, place 1/2 of the overall lift in the opposite shoe as an insert initially. Two weeks later, take 1/2 of that away, then finally 2 weeks later take it all away so you are left with just the desired outsole lift. This eases the process dramatically, allowing the body to relax more in making this big change.
Understand the 3 Measurements taken on a Standing AP Pelvic Xray
Standing AP Pelvis Xray with shoes and orthotic devices
Look at the heights at the Acetabulum, Sacral Base, and the Iliac Crests
As you review this x ray, you will see that the the left hip at the acetabulum (hip joint) is higher than the right. This is the true leg length difference if the foot is in its neutral subtalar position (why it is best to take this xray with stable shoes and stable orthotic devices in the shoes). The symbol marked UPRIGHT means standing and is on the left side. The base of the spine where L5 vertebrae rests on the sacrum, also called the sacral base, drops to the right side. Many feel that getting a level sacral base is more important than correcting the hip height difference.The highest point on the iliac crest, not even seen on the left since it is higher than the right side, is a summation of the pelvic difference. When you look at many points on the pelvis, comparing right to left, you will see how the left is higher all around. However, one of the major problems we face is one of trying to take xrays only when crucial (due to the radiation). I would love to x ray after every change I make, but I must be conservative due to the radiation exposure.
Common X Ray Findings Example:
Hip Height at Acetabulum 10 mm short right (TRUE STRUCTURAL)
Iliac Crest 17 mm short right (further pelvic and Sacroiliac joint collapse)
Sacral Base 13 mm short right (amount spine needs for leveling)
With these findings, it is easy to start with 1/8th inch lift (3.3mm) for 2 weeks, another 1/8th inch for 2 weeks, and then 3rd 1/8th inch lift for the final 2 weeks. I start with tie-on shoes that take the full 3/8th of an inch. I would then have the patient wear this amount for two months to get use to them. Some time with a physical therapist to work out the predictable muscle soreness that will ensue would be great during this time. After the 2 months, if there is still limb dominance, still some symptoms, then I would go up another 1/8th to correct for the sacral base (the extra 3 mm the xrays showed). Of course, many stop the correction at lower levels if the symptoms are resolved. Patients can fight you a lot during lift therapy since they do not want lifts. Who would?? It is important to stay focused, and the xrays really help in this regard. The xrays tell us what is the short side, and by how much. Treatment can be gradual, but complete correction of a short leg is usually obtainable. Watching walking and standing habits you can see these gentle habitual leans (dominance) that can be a sign of short leg syndrome.

Gentle lean to the left of the girl standing noted