This is a simple, but often effective, wrap for various forms of metatarsal pain including Morton's Neuroma. Readily available 2 inch Kinesiotape or Rocktape, and small Hapad metatarsal pads can be used. Purchase Kinesiotape from Amazon and go to www.hapad.com. Hope it helps you. Rich
Monday, January 26, 2015
Sunday, January 25, 2015
Calf Strain: General Treatment Thoughts
Lower Calf Strain
by Richard Blake, DPM

The lower calf above the achilles tendon is comprised of the big calf muscle fibers (gastrocnemius) and the lower smaller soleus fibers seen more to the side in the photo above but going into the tendon
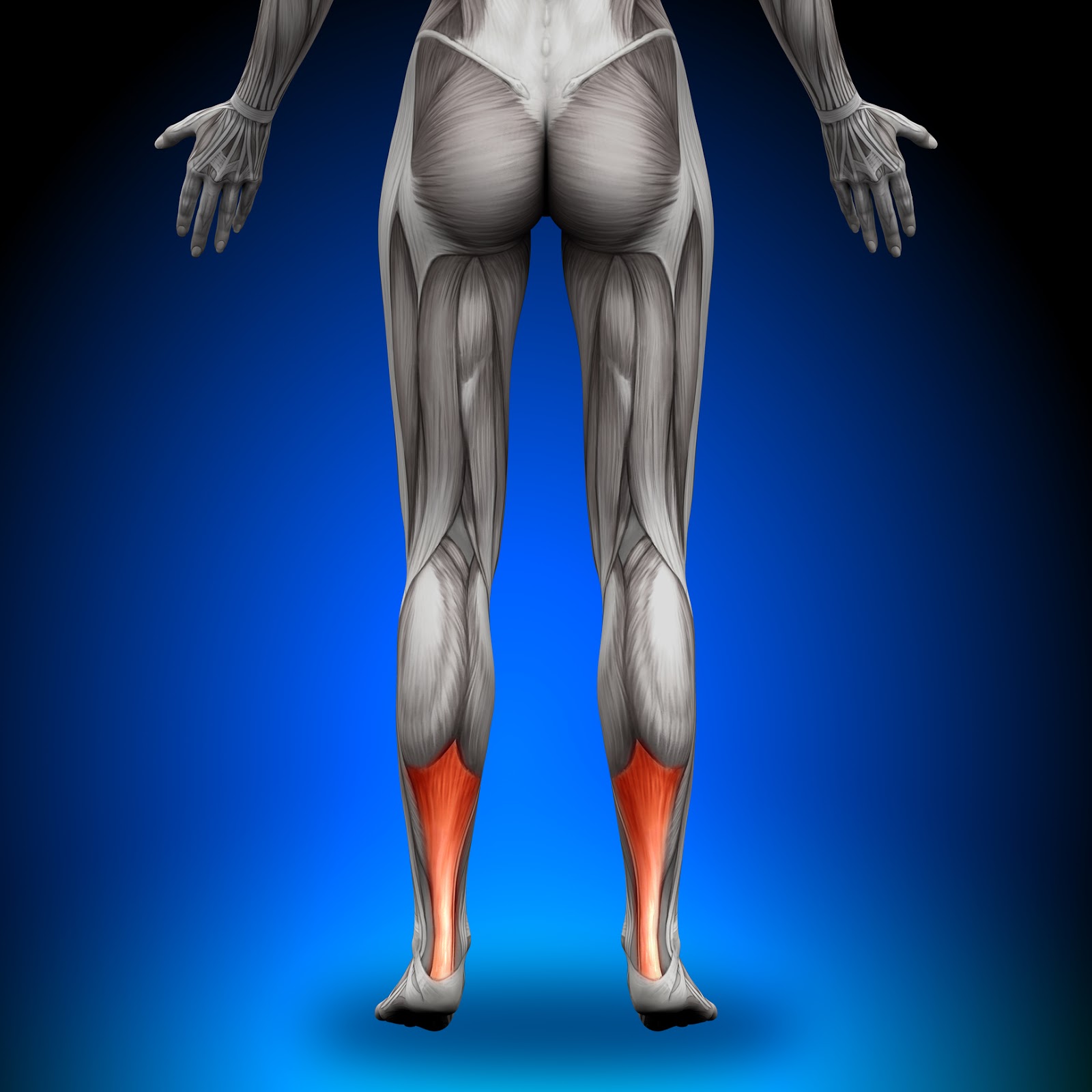
The lower calf is the beginning of the merging of the calf muscles (gastrocnemius and soleus) before the start of the achilles tendon
The top 10 treatments for lower calf strains are:
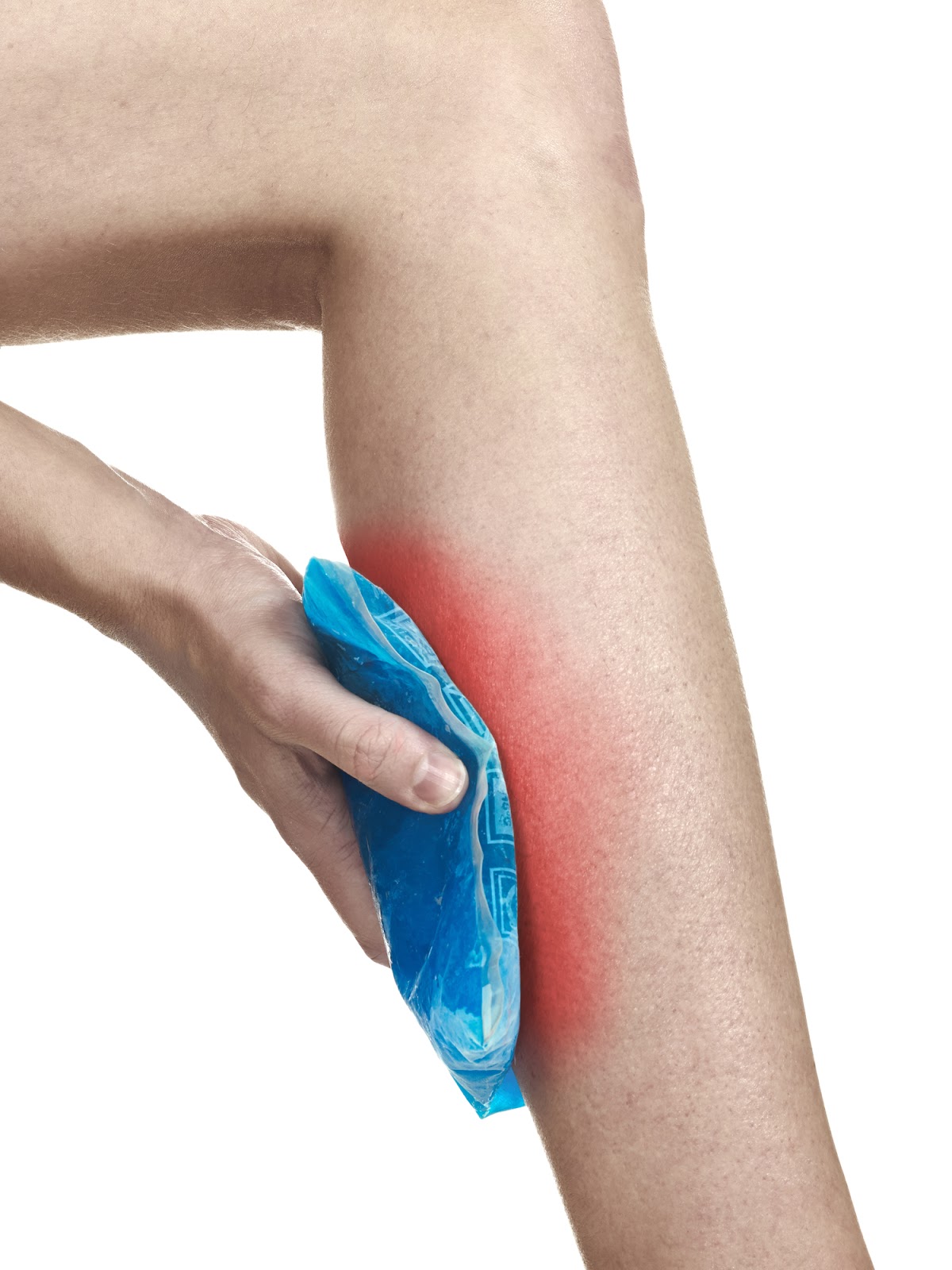
1. Ice pack or massage for 10-15 minutes three times daily initially, and then following activity that may aggravate.
2. Avoid non supported heel positions/activities until the pain resolves and the strength returns (like getting off your seat in cycling, etc, except perhaps the downward dog in Yoga).

3. Begin re-strengthening the calf muscles as soon as injured, but avoid negative heel positions. Use theraband resistant bands knee straight and bent first, and after building to 2 sets of 25 reps, begin 2 sided calf raises.

Theraband for soleus strengthening ankle plantarflexed knee bent

I love starting with 2 sided toe raises (calf raises) but do not drop your heel below the plane of the front of your foot.
4. Stretch the calf by doing the 3 achilles stretches 3 times daily. Go to YouTube and type drblakeshealingsole achilles stretches and you will find them demonstrated.
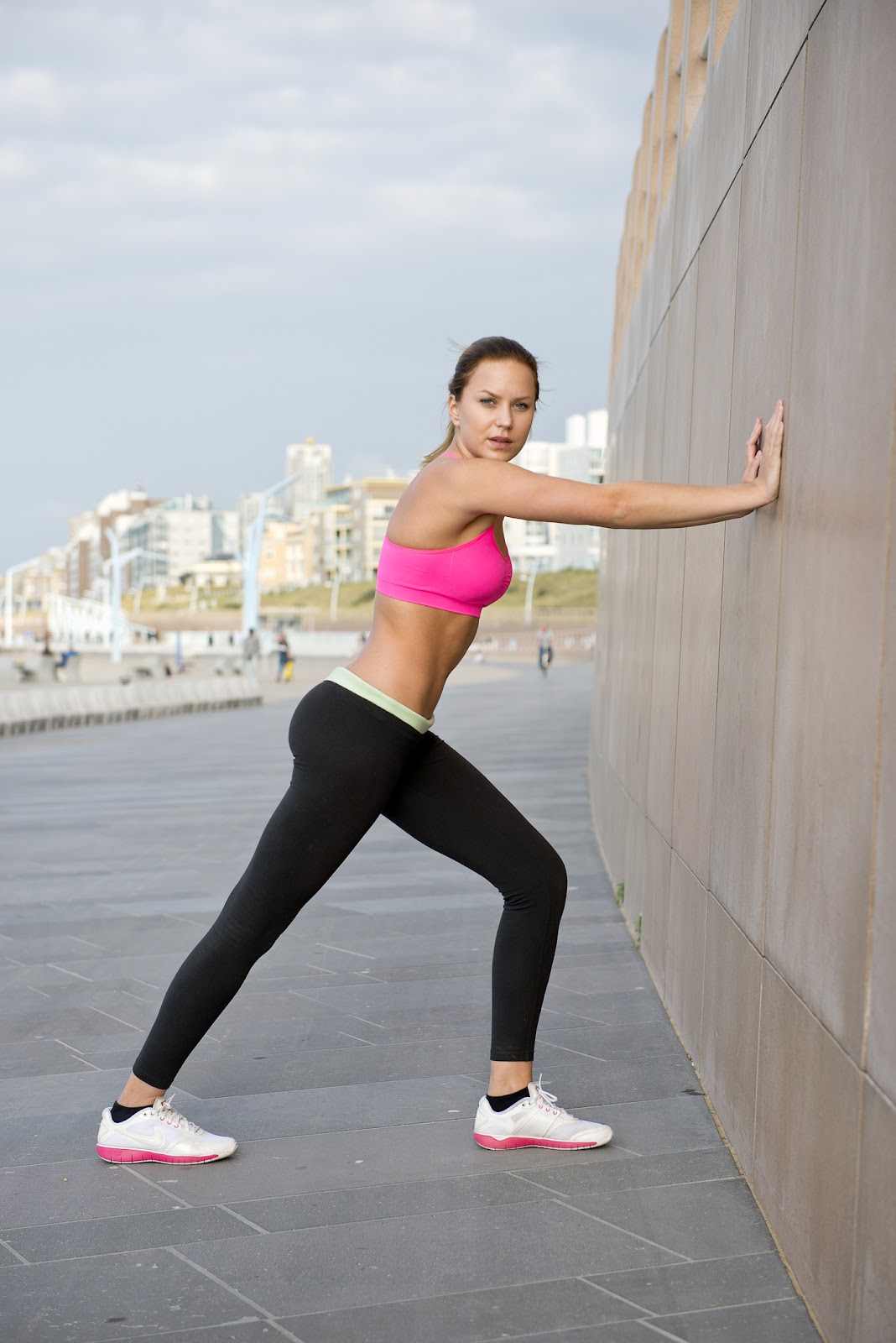
Here the heel is on the ground perfectly for the initial knee straight stretch for the gastrocnemius.
5. Various forms of taping can help take tension off the muscle

6. Deep calf massage is crucial for many calf injuries and 6-8 sessions is typically enough. You can begin this process with massage sticks and rolling pins for self massage. You need to find those trigger points and work them out.

7. Avoid barefoot as much as possible initially, and consider heel lifts (¼”) and clogs or stable heels to relax the calf.

8. Have your achilles flexibility tested when/if you go to PT since many patients actually have too flexible tendons and should not be stretching.
9. Create a pain free environment even if a removable boot is necessary. For calf problems, the boot must go to just below the knee and use an EvenUp for the other side.

10. If the initial injury had some black and blue (ecchymosis), you should try to get to physical therapy sooner than later to help lessen the overall scarring that can settle in and be stubborn to remove.
Friday, January 23, 2015
Hallux Rigidus: Cheilectomy, Implant or Fusion
This is a nice review of current thoughts from the surgical standpoint on Hallux Rigidus. I am remiss at telling my patients what stage they have, and the article makes distinctions between Stage 1, 2, 3, and 4. I believe the conservative treatment in Stages 3 and 4, the so-called surgical stages could probably be better, with less going to surgery. I do not have a magic formula, but have so many patients in these phases who are trying to avoid surgery, especially if fusions is their only option offered. This article does give a valid argument towards joint replacement before fusion, which I am happy they considered this.
Accessory Navicular: General Treatment Thoughts
Accessory Navicular Syndrome
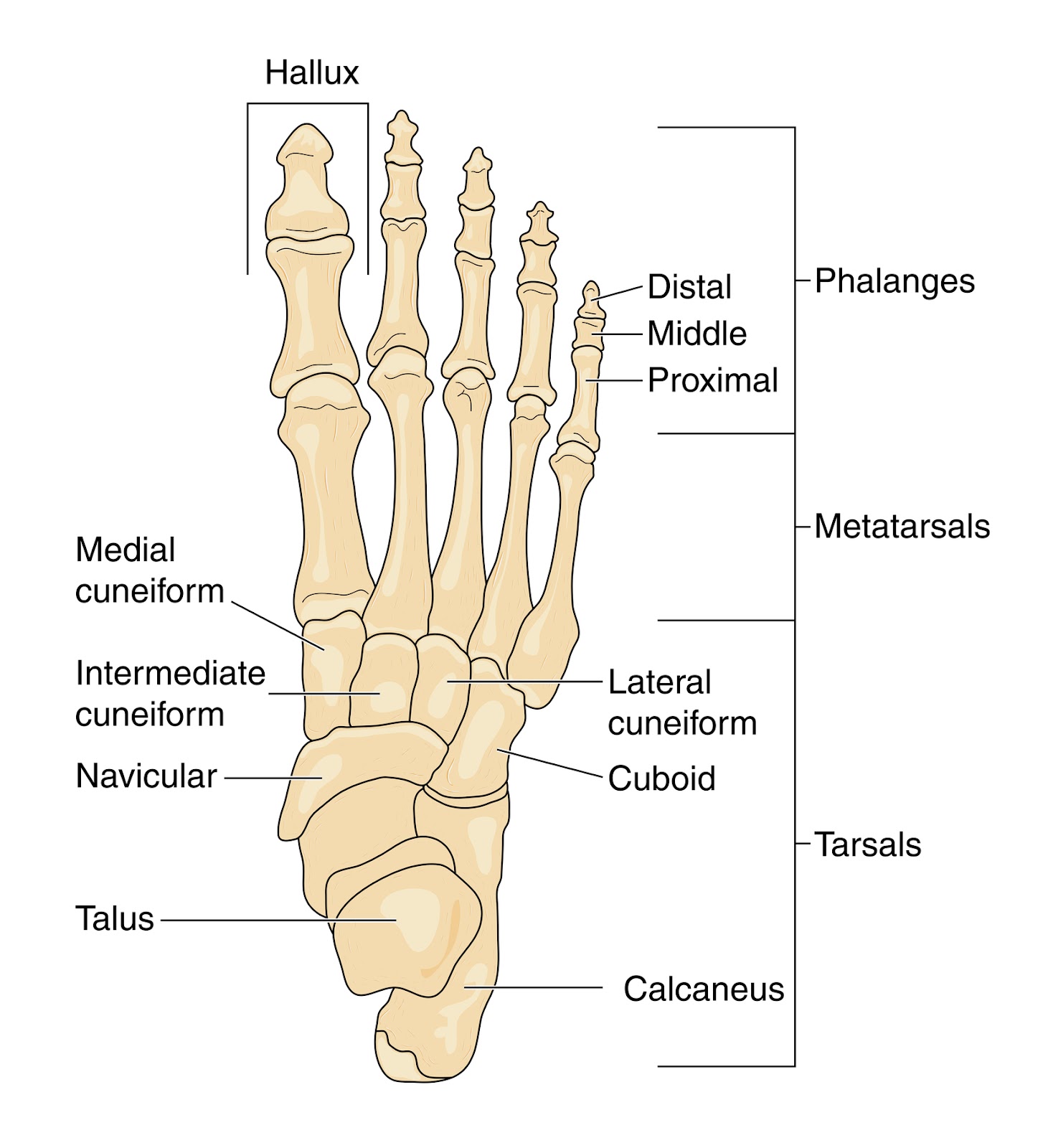
The accessory navicular would be next to and to the left of the navicular. It can be so big that it looks like a second ankle bone.
Here I am separating posterior tibial problems from a unique problem which occurs where the posterior tibial tendon attaches into the navicular. From that point, the navicular spreads under the midfoot supporting the arch with multiple attachments. When you have an accessory bone where the posterior tibial tendon attaches (around 3% of the population) much of the force is lost that supports the arch. The normal tendon attaches into the extra bone, which has little to no arch support function, instead of where it should go. A syndrome of pain, arch collapse, and mystery can occur. The mystery is that at times the accessory bone needs to be removed, but most of the time you can co-exist with it (95% of the time). Even in the 5% that need surgery, it takes a lot of time trying to avoid surgery to find those that really need it.
The top 10 treatments for accessory navicular syndrome:
1. An MRI is very important to discover what the source of pain actually is: stress fracture, joint inflammation, or tendinitis. There is a joint between the navicular and its accessory bone.
2. Use Kinesio Taping or supportthefoot.com tape or classic low dye taping techniques intially 24/7 and then for extended activities.
3. Ice pack the sore area 10-15 minutes 3 times daily.
4. Go into a removable boot (such as an Anklizer) for 2-3 months if needed to calm the foot down.
5. Strengthen the posterior tibial tendon starting initially with active range of motion like ankle circles.
6. Check out the Aircast Airlift PTTD brace to see if it is helpful for you and can get you out of the boot faster.
7. Custom foot orthotics are a must for a 2 year period. They must produce a good force against the navicular, but it may take time finding the right orthotic guy/gal.
8. You can use Sole OTC orthotic devices with medial longitudinal Hapads initially until a good protective orthotic device is made.
9. Create a pain free environment as soon as possible (level 0-2).
10. If the MRI shows bone reaction (edema), order a bone stimulator as soon as possible to start strengthening the bone.
Email Correspondance:

Dear Dr. Blake, I was wondering if you would be able to clarify some information to help us make some smart treatment decisions. My 13 year old daughter is a high level soccer player. She started to complain of pain in her foot last spring during the time she played soccer and ran track. She also played in 14 games of soccer without ever coming out. A significant increase in activity. The pain was located on a bump that has been recently identified as an accessory navicular. She was first treated with rest and 4 weeks of physical therapy and orthotics. After returning to sport the pain returned but was slightly higher above the ankle. MRI shows no fracture but edema indicative of stress changes in the os naviculare.
Dr Blake's comment: The edema/swelling seen within the os navicularis/os tibial externum/accessory navicular can take months and months to resolve after the initial injury, so not an indication that things are not healing. The pain above the ankle was one of the tendons trying to help out the injury: FDL, PT, FHL, or AT. When one area is injured, the surrounding muscles/tendons help out and do some extra work. That can make them hurt also. A Rule of Three tends to occur until the body re-establishes equilibrium---original problem, compensatory problem #1, and compensatory problem #2. The true injury is at the bump with the accessory bone however.
Dr Blake's comment: The edema/swelling seen within the os navicularis/os tibial externum/accessory navicular can take months and months to resolve after the initial injury, so not an indication that things are not healing. The pain above the ankle was one of the tendons trying to help out the injury: FDL, PT, FHL, or AT. When one area is injured, the surrounding muscles/tendons help out and do some extra work. That can make them hurt also. A Rule of Three tends to occur until the body re-establishes equilibrium---original problem, compensatory problem #1, and compensatory problem #2. The true injury is at the bump with the accessory bone however.
Current treatment is 6 weeks non weight bearing air cast, then progression back to activity. She has so far missed 4 months of training. Everything we seem to read is confusing relating to surgery vs conservative treatment. For a high level athlete looking at missing another 3-4 months is devastating. We are wondering if surgery would be a better option as everything we seem to read indicates non surgical treatments are not effective.
Dr Blake's comment: I am sorry the literature is so poor on this subject. Yes, some patients need surgery. Doctors have a hard time deciding on surgery on someone that age, so feet get dragged.
Dr Blake's comment: I am sorry the literature is so poor on this subject. Yes, some patients need surgery. Doctors have a hard time deciding on surgery on someone that age, so feet get dragged.
It is an impossible decision for a parent to make, since surgeries can have problems, and the patient can be worse (less than 10%). When they are worse, there is usually an explanation, but a second surgery is often needed after months and months of unsuccessful rehabilitation. For a professional athlete, paid big bucks, they have surgeries for speed of rehabilitation. Every second they miss playing cost the team money. But, in the non professional, and at a young age, you want to be very very sure that surgery is needed. I have treated 100s with this condition with less than 1% having surgery (and perhaps another 9-10% just stopping their activities to avoid surgery). So, 90% get better without surgery and can continue with their sport of choice at a high level, will your daughter be one of those?
Our doctor indicates feels that the literature supports good outcomes with nonsurgical treatment and that is what she recommends. Any information you can share to help us would be great. We just want to make sure that whatever treatment she receives limits the time out of sport and reduces the chance of recurrence.
Dr Blake's comment: The approach to getting this better, and keeping it better, is a multi-discipline approach.

The podiatrist/therapist/orthotist must make great orthotic devices to stabilize the injured arch/accessory bone. The physical therapist/trainer must develop a strengthening program, pain free, that gets the posterior tibial tendon, and the surrounding muscles/tendons, and the quads/core strong as the other side. Your daughter should be icing twice daily and contrast bathing for the bone edema once daily to remove the inflammation. She should be on a stationary bike, etc, pain free, up to one hour per day to get the legs strong for her return to activity. She needs to learn the best way to tape the area which gives her the best pain relief, since taping in soccer games/practices is crucial and more protective than orthotics. She should be in the deepest soccer shoe she can find. It is when the orthotics, tape, strength, pain level are right, she can go back to activity. The coach is probably the most vital part to this team.

She/he must be protective of your daughter, be vigilant for signs of limping, know when to rest her, when to play her, perhaps change positions temporarily to help the demands on that ankle/foot. If the coach can not do this, all our best plans are destroyed, and it gives conservative management a bad name. Make sure diet is very healthy, including at least (2) 4 ounce servings of red meat weekly, if she is not a red meat eater.

And, as parents, you need to get rid of any timeline right now as you read this. Honor her body tissue. Do not think about timelines, you will only get frustrated. Thank you so much.
So, in summary, here is your next 3 month assignment: Wean from Non weight bearing to weight bearing without increased pain.
- Perfect the orthotics
- Perfect the soccer cleats
- Avoid barefoot at home if that bothers the area
- Learn a variety of taping methods
- Ice and Contrast Bath daily
- Eat healthy
- Talk to the coach about a gradual return to soccer, and any ideas on position change
- Tell the physical therapist you want to learn a pain free gradual and progressive strengthening program so 6 months from now you/she have tendons of steel (at least 3 times stronger). Good Luck!!

And the response:
Dr. Blake,
Thank you so much for your information. As a result of the info you provided we decided to seek a second opinion from an orthopedic surgeon. His diagnosis correlated with your info. He recommended casting in a walking boot for the next 3 weeks but did not feel NWB was necessary or appropriate. This is great news for us as this is not a stress fracture of the navicular as we were being told was a possibility as well . She is allowed to walk in the boot and swim which will decrease unnecessary deconditioning and ankle stiffness. He also said surgery may be an option using a modified kidner only if conservative measures fail. He recommended physical therapy and orthotics. Thank you again. It is nice to finally have a clear diagnosis and logical treatment options backed by two professionals.
Accessory Navicular: An Accessory You May Want To Do Without
This email was received from a patient suffering from a syndrome of pain produced by a weakened attachment of the posterior tibial tendon into the navicular. The posterior tibial tendon is the strongest supporter of the arch. The weakened attachment is due to an extra bone next to the navicular at the height of the arch. This extra bone occurs in probably 3% of the population and is called accessory navicular, os navicularis, os tibial externum, and the extra ankle bone. In only 10% of those patients with it does it occur on the other side also (bilateral).
Hello Dr. Blake,
I am a 29 year old who has been suffering from a lot of foot pain since early childhood-- it wasn't until I was in highschool that the Dr. examined me standing and realized that my arches "collapse". Finally they took an x-ray and found that I have bilateral accessory naviculars. I have since worn orthotics and attempt to wear very stable shoes (i.e. Saucony Hurricane). Due to the pain, I cannot do high impact sports, and walking long distances usually results in pain and limping. (I will also get shooting pain up my shins, in my knees, or in my thighs/hips). There are not too many shoes I can wear comfortably, and even with my orthotics I will have pain if I walk
more than a mile or so.
 |
X ray shows accessory navicular under the navicular at the height of the arch.
|
Dr Blake's Note: The os tibial externum begins to form around 8-9 years old, and should be fully formed at 16 years old. It can fully attach bone wise, or partially attach with cartilage or fibrous tissue. These last 2 attachments are particularly weak and can cause pain.
 |
This MRI view of an Accessory Navicular shows it inferior and closer to the heel than the big toe.
|
In the past, my foot doctor has suggested that if pain cannot be improved with orthotics, I should consider having them surgically removed. The Dr. mentioned that most people have pain from the bones rubbing on shoes, etc, which I have never found rubbing to be a problem, more like pain from misalignment. I did PT for a while, and much of the focus was on stretching and strengthening muscles, especially my hips. While this did help with aches in knees/hips/thighs at the time, I don't really feel like my overall strength or balance has improved.
Dr Blake's Note: I have never had a patient with this syndrome with pain limited to shoe rubbing, since orthotic devices, shoe padding, and taping all take the pressure off the outside of the bone. The real pain is from something else, and that is what needs to be discovered . Discovering where the pain is coming from hopefully will enable the patient to avoid surgery, since the treatment can be directed at that, or if surgery is necessary, make sure the right surgery is performed.
I also have very poor balance, tight achilles tendons and hamstrings,
and weak muscles.
Dr Blake's Note: If you read the discussions later on posterior tibial and arch strengthening, you will understand the complexity to strengthening through pain. If the tendon is damaged, you will not be able to strengthen it, and surgery may be necessary. If the tendon is not damaged, it is vitally important to attempt to isolate it and strengthen it, pain-free, and not strengthen the peroneals at all.
I also apparently have possibly pinched nerves between my big toe/second/possibly third toe at times when walking-- the area above and between by big and second toe will swell a bit and I get tingling/pain//numbness in my third toe sometimes when walking.
Dr Blake's Note: The significance of this statement is that Lindsey may have a version of Tarsal Tunnel syndrome which gives posterior tibial symptoms, and also superficial toe nerve symptoms. This would be a rare situation, so I will ignore it right now, but keep the info somewhere in the recesses of the brain.
Recently, I made the silly mistake of wearing sandals to the mall. After walking around, my right foot began hurting, and has been getting worse (now on day two). The pain is located directly below my ankle on the inside in a very localized spot, and has been swollen. I have been icing it and it helped minimally (I also tried tylenol). It hurts regardless of movement, bearing weight, etc.
Dr Blake's note: also perhaps Tarsal Tunnel??
Dr Blake's note: Like many of these chronic problems, they can become acute at times. The mistake made now is not to recognize that you have to treat this acute injury first, and deal with the chronic injury after. Lindsey is now in the Acute Phase of Rehabilitation (for this chronic injury). The treatment is immobilization and anti-inflammatory. Get yourself into a removable Anklizer Boot and ice 3 to 4 times a day for 15 minutes. If the ice irritates the local nerves, ice 3 inches above the area, and consider a Rx of voltaren gel 4 times daily or Flector Patches every 12 hours. Should be better in 1 to 2 weeks.
I tend to "hold my arches up" and transfer more weight to the outside edges of my feet, because letting my arches collapse immediately causes pain and irritation.
Dr Blake's Note: This is what the orthotic devices must do for a patient. They must be designed to hold up the arch, perhaps along with Kinesiotape, so that the patient doesn't strain the tissue further doing it using muscles and tendons abnormally.
I was told by my Dr. that the tendon holding my arch up is partially connected to the accessory navicular, making my arch unstable and collapse. ( I have also been told in the past that I have "loose ligaments-- but I have noticed that while I am very flexible in some joints, I am extremely tight elsewhere).
Dr Blake's Note: If you imagine that only 1/2 of your achilles tendon attached where it should, and the other 1/2 attached into a soft ligament, you would not have only 1/2 the strength, you would have next to nothing. As the achilles pulls, the weakest link in the chain (the part not attaching into solid bone) would begin to strain, and the whole achilles begin to hurt. Same with the accessory navicular, the part of the posterior tibial tendon that does not attach into solid navicular begins to strain trying to stabilize the foot, and slow down pronation of the foot, ankle, knee, sooooo pain ensues. It can not do it's job properly.
I am not sure what sort of direction is best with this problem. I don't know if this swelling/pain is from the extra bones and would diminish with surgery, or not. The pain is so frustrating and keeps me from being active too much at all-- I enjoy dance, walking, yoga, cycling and swimming-- but often walking and dance are limited (and running is out of the question) due to the pain it will cause.
Dr Blake's Note: Once the acute pain is gone, and you are back to dealing with only chronic pain, you need to get this worked up. I will give my final recommendations below, but you must know my recommendations center around a world that I would like, maybe not practical.
It seems like my pain is not the usual for accessory navicular (as according to Dr.) so I am not sure if this is an unusual case? Any advice or information on this would be great. This has been causing trouble for most of my life (i.e. being unable to enjoy walks/hikes/sports, having trouble falling asleep due to pain, pain and limping at work).
Thanks,
Lindsey
Lindsey
 |
MRI view on the partial bone attachment of the accessory navicular.
|
Dr Blake’s response:
Lindsey, Most of the pain from this syndrome can be from inflammation at the attachment of the posterior tibial into the accessory navicular, actual tearing of the tendon itself, injury to the spring ligament just under this bone, chronic movement of the accessory bone on the parent bone (navicular) like in a fracture non-union, or originating from another structure (both tarsal coalition and tarsal tunnel syndromes can have similar presentations at times). Please read the section entitled Tip of the Iceberg since sometimes the apparent problem is actually not what is producing pain. You are definitely a surgical candidate due to the length of time you have had this. That being said you need a good work up to make sure they operate on the right area and do the right thing for you. And, you may find along the way that you don't need surgery. So, if I could prioritize wish lists for you, they would like this:
- Get the acute pain calmed down with an Anklizer Boot, an EvenUp for the other side, anti-inflammatory. You will need the boot and EvenUp again.

- Get an MRI to look at the tendon, attachment of the bones, spring ligament, tarsal coalition, and tarsal tunnel areas.
- If the MRI shows a lot of bone activity, get a bone scan.
- Talk to a Physical Therapist about isolating the posterior tibial tendon during strengthening. Can you do at least isometrics without pain? Begin strengthening the tendon, same exercises are needed post operatively. Strengthening should only be done in the hour before bed, and ice after even if it does not hurt.
- Get an orthotic that is comfortable, but supports your arch. Are there doctors or therapists in your area that use a version of the Inverted Orthotic Technique? You must feel that the orthotic works so well that you do not need to pull up your arch.
- Ice three times daily period. For 15 minutes each. Since you can wrap ice around the top and inside of your foot and walk around the house, at least you can do other things.
- Learn to Kinesiotape your arch or check out the tape from suportthefoot.com. Tape daily. You can ice through it.
- Do not go around with sandals or barefoot. Dansko clogs may work. A compromise may be an Orthaheel or Chaco Sandal with Kinesiotape.
- Feel free to send me any tests along the way. You have a big journey. Hang in there. Be Logical. I hope this has helped. Rich
Thursday, January 22, 2015
Cheilectomy Post Op: Patient Shares Post Op Course
Comment Posted January-22-2014
I am 2 weeks post opt rom having a cheilectomy done on left foot. I am pretty pleased with how it is going and am in a soft shoe most of the time. 13 staples taken out 3 days ago and this seems to be quite sensitive where these were taken out and healing is slow. Hoping in 2 weeks I have greatly improved by then. Less is more for this type of problem and my doctor feels a fusion is last option to consider.
I'm 49 year old female very active and a runner so will keep you posted on my recovery. My hallux rigidus was quite bad and it was time to do something about it. Good luck everyone and if I can be of any help let me know.
Dr Blake's comment: This kind patient is post cheilectomy for Hallux Rigidus. She has agreed to respond to comments or questions. I am very appreciative.
Hallux Limitus/Rigidus: Comment on Self Mobilization
This is a comment on the below video on my YouTube channel ---drblakeshealingsole
What if you have arthritis and some bone spurs and it hurts to do this? Will this make it worse? thanks
And my response:
Thanks for the comment. The force you generate should not hurt anything, but you do need to do it painlessly. If there is pain, then after the activity, the body tends to tighten the joint even more. Some patients have to use warm water soaks before, or at least move the toes around, to warm them up before the mobilization. Also, if it hurts please ice for 5 minutes after to neutralize the possible irritation. Dr Rich Blake
Wednesday, January 21, 2015
Plantar Heel Bursitis: General Treatment Thoughts
Plantar Heel Bursitis
A bursae is a sac between the skin and bone that, if the area is traumatized, can fill up with fluid (called bursitis) to protect the underlying bone. Bursitis is common in the feet, knees, hips, elbows, and shoulders. I once had 7 months of shoulder bursitis from incorrect biomechanics while painting a cathedral ceiling in my house. Plantar heel bursitis is often confused from plantar fasciitis. Acute plantar heel bursitis can develop suddenly from impact, but a bursitis can also develop slowly from chronic inflammation (typically secondary to plantar fasciitis or calcaneal bone injuries. If you have plantar heel bursitis, you typically can not walk on your heels without pain. Having my patients first walk down the hall barefoot normally, then on their toes, and then on their heels only, can make the diagnosis of bursitis (although a small stress fracture on the heel bone make still be present. One of the treatments for heel bursitis (not initially) is a cortisone shot. Because the bursitis can be secondary to something else that the shot may hurt, I try not to do a shot unless I have an MRI if possible. And, sometimes, you just have to take your chances if it does not make sense that anything but bursitis exists. Always consider that you make have a bursitis, with plantar fasciitis, if treatment of the plantar fascia alone is not helping.

Elbow bursitis (aka students bursitis from chronic leaning on elbows while studying. Many times heel bursitis looks like the skin wants to explode releasing the fluid trapped.
The top 8 treatments for plantar heel bursitis:
1. 5 minute frozen sport bottle roll just under the heel 3 times daily
2. Heel cushions to protect the heel (sometimes used alone, and sometimes an arch support to transfer weight off the heel is vital)
3. Physical therapy to breakdown the bursal sac with a combination of ultrasound to super heat, deep tissue massage to break down or move fluid, and electrical stim to push fluid out.
4. Cortisone shot, if the above is not eliminating problem, and a MRI has ruled out any other problem. These shots are given from the side of the heel, not from directly under, which makes them less painful. A series of cortisone shots may be necessary (see the section on cortisone shots). This is the only heel pain diagnosis that a cortisone shot is used for.
5. Avoid barefoot for continual irritation
6. Use some heeled shoe, like a dansko clog, around the house.

7. Use wedges instead of straight heels to distribute the weight better.

8. Also, consider wearing Crocs for their shock absorption

Heel Bursitis (Plantar/Bottom of Heel): Typical Physical Therapy Regimen
Hi Dr. Blake!
I hope you have a fun-filled long weekend planned!.I'm checking in at the two week mark as we discussed. My stubborn little calcaneal bursitis is still causing me grief. I did try the contrast bath - but it seemed to irritate it, so I've stuck with icing. I have not been jumping in dance class or standing in spin. In fact, releve (going up on the ball of the foot) seems to bug it as well, so I've eliminated turning. Since I wasn't making the progress I'd hope to on my own, I thought I'd finally book the PT. I work in SF, so I would consider coming over to St. Francis, but if you know of another good place in the East Bay, it might be more convenient.Thanks so much! It really is wonderful having someone I've known for 24 years (!!) I can come to with these bothers. And even though it's an injury that brings me in to see you, it is always great to see you! ;-)
Have a fabulous weekend and talk soon,
Tracy
Dr Blake’s response:
Tracy,
Physical Therapy for calcaneal bursitis (under the heel) should be done twice weekly for 4 weeks and should include in this order: Ultrasound as a way of producing deep heat to the bursitis tissue making it vulnerable to the next two treatments. The ultrasound is following by deep friction massage to break down the bursae. The deep tissue work is following by 5 minutes of vigorous ice massage to calm down any aggravation of the inflammation and further the breakdown process. Since plantar fasciitis is normally part of the problem, the PT may address part of the treatment for that also. If calcaneal bursitis is a major part of the pain, make sure that the 3 components in the order of ultrasound, deep friction massage, and icing are the central part of the treatment. I will see you following the first 4 visits to make sure we are all on the same page. Good luck, and great to see you again as always. Rich
PS. During the time you are in physical therapy, you must continue to ice massage 3 times a day (since the contrast bathing did not help), and do as much physical activity as you can without flaring up the symptoms. It is normally a mistake to go to physical therapy at the same time you are resting an injury completely. The physical therapist never gets a good feel of your improvement, or lack of improvement. Use the information on Good Pain vs Bad Pain to base your Activity Modification Program.
Also, the next step with calcaneal bursitis is cortisone shots, but that requires 2 weeks off activity/shot, and could require up to 3 shots (the response to the shot is evaluated in 2 weeks), so most athletes try to avoid with a passion. Good luck Tracy, email me after 4 physical therapy visits.
Tuesday, January 20, 2015
Chronic Pain: Chronic Opioid Use may not be helpful
This was sent to me by a colleague who deals with chronic pain patients and tries hard to find ways to avoid long term opioid therapy when possible.
Highlights findings from NIH's panel:
There's Scant Evidence for Long-Term Opioid Therapy in Chronic Pain.
"We don't know enough about who benefits from opioids and who doesn't, about who gets pain relief and who gets into trouble with adverse effects from these drugs."
It's also not clear which pain types respond to opioid therapy. "There are many different kinds of pain and some pain perhaps responds better than others.There's a huge gap in knowing which is the right hammer for the right nail."
Chronic pain affects an estimated 100 million Americans or a third of the US population. About 25 million have moderate to severe chronic pain that limits activities and diminishes quality of life. Pain is the main reason Americans receive disability insurance.
Experts estimate the societal costs of pain at $560 billion to $630 billion per year in the United States due to missed workdays and medical expenses.
To manage pain long term, some 5 to 8 million Americans depend on opioids.
From 2000 to 2010, the number of hospitalizations for addiction to a prescription opioid increased more than 4-fold to more than 160,000 per year.
When it comes to managing patients with legitimate pain conditions, physicians have little training. They're sometimes quick to label patients as "drug-seeking" or "addicts," and some even "fire" patients for merely voicing concerns about their pain management, the report notes.
"A more holistic approach to the management of chronic pain that is inclusive of the patients' perspectives and desired outcomes should be the goal," they write.
Because pain affects physical, emotional, and cognitive function, as well as interpersonal relationships and social roles, managing pain requires a multidisciplinary approach similar to that recommended for other chronic complex illness, such as depression, dementia, eating disorders, or diabetes.
Treatment for Short Leg Syndrome in Child: Email Advice
Hello Dr. Blake,
My son has seen you several times for orthotics. He was diagnosed with cerebral palsy, has bilaerally pronated feet, and mild scoliosis.I don't like to x-ray him often to reduce his exposure. I want to get an accurate x-ray that eliminates other factors that might be impacting what is seen on the x-rays such as standing posture, pronated feet etc., in the hopes that I can see how much of it is his spine and how much comes from these other factors. I hope that in this way, we can try to address these other factors individually and their impact on the spine, of course with the goal of correcting his scoliosis.
Dr Blake's response:
Thank you for the email. I agree to be mindful of x ray exposure, but you also have to have accurate information to treat your son. Typically, once the orthotics are where I like them, I have the patient take an AP Standing Pelvic Xray with orthotics on but no lifts. I coach the patient to stand as straight as possible daring the xray to show a short leg. The xray gets the leg length difference, any pelvic rotations, any unevenness of the base of the spine, and also the lumbar part of the scoliosis. Since it is weight bearing, it has a true bearing on how he walks. After I review the xray, I will make recommendations on lifts, physical therapy, etc. I love sending patients who have pelvic or sacral base unevenness to Dr Irene Minkowsky here in San Francisco. She typically knows what profession can help the most. Hope this makes sense. Rich

Sunday, January 18, 2015
Ankle Joint Instabilities: General Treatment Guidelines
Ankle Instabilities
When you sprain an ankle ligament, or any ligament that stabilizes a joint, you always get some mechanical instability. This instability can be tested and documented by physical examination or stress x rays. But, it is functional instability that is the most important to treat. When patients sprain their ankles or knees, we try hard through strengthening exercises, bracing, and occasional surgery to remove functional instability. Functional instability feels like the joint shifts or will give out or does give out. With functional instability you have true disability. A wonderful paper written in the 1960s by a Dr Freeman clearly showed if patients could learn to balance on one foot post ankle sprain that their need for ankle ligament repair was almost zero. This paper heralded in the concept of using tendon strength to overcome the loss of ligament integrity, at a time when primary ligament repair was commonplace post sprain.

The top 10 treatments for ankle instabilities are:
- Re-strengthening of the muscle/tendons in the area that would protect the side of the joint of the ligament loss.
- Single leg balancing with gradual progression of difficulty
- Various ankle braces
- Various forms of ankle taping

- High top shoes for various activities like backpacking on uneven terrain

- Custom made orthotic devices to stabilize for the injured ligament
- Consider Prolotherapy (injections into the ligaments of sugar water)
- Strength the muscles/tendons above and below the injured ligament to help with the overall function.
- Control the overall swelling in the area which adds to the instability
- Surgical consultation to see what the process and prognosis of surgical repair
Subscribe to:
Posts (Atom)