Morton's Neuroma: General Principles
by Richard L Blake, DPM

The top 10 initial treatment options for Morton’s Neuroma are:
- Attempt to off weight the painful area with a metatarsal pad
- Ice pack the bottom of your foot for 10 minutes 2-3 times per day
- Begin using a topical nerve medication like Neuro-Eze or compounding medication
- Do neural flossing three times per day
- Avoid barefoot walking until the symptoms begin to resolve
- Experiment with shoe gear that seem the most comfortable (not necessarily what you think)
- Look into other causes of nerve pain like sciatica or tarsal tunnel
- Do what you can to create the pain free environment (0-2 pain levels)
- If the metatarsal pads does not help, see if you can get fitted for orthotics or Budin splints
- If there is any swelling, each evening do contrast bathing
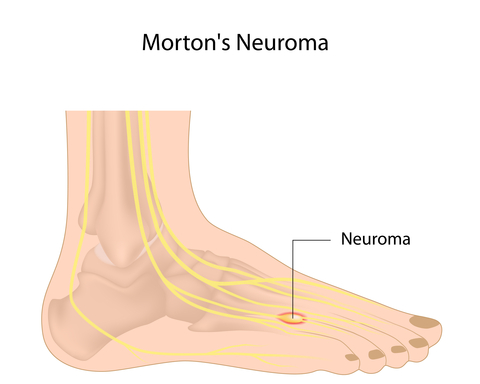
Morton’s Neuroma denotes a swollen inflamed painful nerve classically between the third and fourth metatarsals, radiating into the third and fourth toes (toes are numbered one for the big toe and 5 for the pinky toe). It can also be between the second and third metatarsals, or between both the third/fourth and second/third just to make diagnosis more difficult. The nerve symptoms created can be more like numbness, tingling, buzzing, burning, sock rolled up sensation, etc on one side on the spectrum, to sharp, radiating, and electrical pain at a level 8 to 10 on the pain scale. One of my unfortunate patients described it as lava flowing in her foot!!
One third of all patients only have numbness as the chief complaint, one third have a combo of numbness and some pain, and one third have only pain (lucky them!!) The pain can be so bad that the differential diagnosis could only be a broken bone, however the history of onset of pain does not match up with a fracture, and there is no swelling. Neuromas rarely have swelling, unless the nerve pain has triggered a version of complex regional pain syndrome.
When a patient presents with symptoms of Morton’s Neuroma, the treatment plan should address 8 areas. These are:
Mechanical support behind the metatarsal heads to off load the sore areas immediately in any shoes which produce pain.

Indirect mechanical support should be done for any overpronation affecting the ankle.
Shoe gear changes can be made to minimize daily aggravation (various factors affect each case—amounts of cushion, amount of heel lift, overall flexibility, toebox tightness, shoe stability, and amount of arch support).
Changes in digital (toe) motion with taping or Budin Splints, and toe separators can be helpful.

Tightness in the ligaments and other soft tissue around the toes and metatarsals may need mobilization to free up the nerve.

Anti-inflammatory measures can be helpful to reduce the inflammation around the nerves like icing and contrast bathing. 
Nerve stabilizing methods, like core work, Neural Flossing, and Neuro-Eze can be vital to desensitization of the nervous system.
Diagnostic testing to determine where the source of the pain originates, whether or not there are classic neuromas present (MRIs are best for the back and foot, with the foot MRI needing contrast dyes).

Luckily, less than 10% of patients need to consider for surgery to remove the nerve if their symptoms do not improve well, but the other 90% can have a rocky road getting their symptoms under control.
Remember, first and foremost that this is a nerve problem. Nerve problems hurt more than any other injury. There are more nerve endings on the bottom of your foot per square inch than any where else on the body. Nerve pain goes straight to the brain and is quite intolerable by most. The treatment should be aggressive and multi-factorial. It takes about 1 year of treatment in the recalcitrant cases (slow ones) to decide that surgery should be done. If you are in the unlucky 10% requiring surgery, 50% of you will heal quickly, and 50% will take up to two years to really feel somewhat better (if at all). So, 5% or 1 out of 20 patients with nerve pain still have nerve pain to some degree 3 years after I start treating them. So, try your hardest to be in the 95%.
Remember that nerve pain makes nerve pain by itself. So, the cycle of nerve pain spiraling out of control must be stopped. Golden Rule of Foot: Treat Neuroma/Nerve pain aggressively, or it will decide to stay around. When I first feel symptoms of numbness or pain in the front of your foot, seek immediate help. But, there are so many aspects of treatment that the patient can only do like icing, shoe gear changes, add Hapads, start Neuro-Eze and neural flossing, limit pain producing activities (if there is pain), doing daily self massage, etc. When I first got into practice 34 years ago July 1981, 50% of all neuromas diagnosed were surgically removed. Now, less than 10% are surgerized (my own word!!) so medicine is moving in the right direction on this one.
Neuroma or nerve pain in the foot must be treated at the foot, but it can be caused by irritated nerves from back problems, neck problems, ankle problems, sciatic nerve problems, and peripheral neuropathies (nerve diseases) from diabetes, B12 deficiencies, etc. Even with our most sophisticated workups on nerve pain, the nerve pain can occur 5+ years earlier than the diagnosis. These are some of the neuromas removed, and yet the patient feels little or no improvement. Medicine has to get better in this area.
What should happen in the first 2 or 3 visits (probably over a 6 week period) with a doctor whose diagnosis is Morton’s Neuroma. These are:
1. Begin a program of anti-inflammatory measures, which is done daily, and could involve one or several cortisone shots.
2. Begin to change from all shoes that aggravate the symptoms (take each shoe separately since you may be surprised what feels okay).
3. Avoid barefoot walking.
4. Begin some evaluation of the possible source of the nerve pain (low back evaluation at a minimum with straight leg raise and Tinel’s test at ankle).
5. Add some Hapad or other metatarsal arch support to all shoes that have adequate room.
6. Begin some exercises that relax the tissues around the inflamed nerve (like toe waving exercises and neural flossing).
7. Begin some massage to desensitize the nerve with Neuro-Eze, some heat lotion (i.e. Ben Gay), or warm face cloth wrapped around foot (as long as the massage doesn’t irritate the nerve).
8. Begin controlling pronation if the ankle mechanics could cause pulling on the branch at the ankle (in what they call the tarsal tunnel).
9. Discuss the timing of possible MRI, Nerve Conduction Test, alcohol injections, course of cortisone injections, possible casting in removable boot.
See you and your healthcare provider have some work to do. Work on shutting off the nerve painlessly, and as quick as possible, before the symptoms get worse.
Morton's Neuroma: Successful Surgery after conservative therapy failed
This was a wonderful comment to my blog (drblakeshealingsole) post below on Morton's Neuromas and their Treatment Options. Thank you to the young man who wrote this. It does not change my mind on being conservative, but I do not think his first 2 podiatrists gave him an option of surgery. I do not do surgery, but we have 2 highly trained surgeons in the office who I consult frequently. If you have a solid diagnosis of Morton's Neuroma, you must be informed of your options, for it is the only way to make the best decision for you. You are the one feeling the pain, the doctors can not, but the doctors should help you stay objective and help you work through the treatment.

Dear Dr Blake:
I had MN in my right foot. I visited three podiatrists before finding one who was willing to perform the surgery - and he changed my life by doing so. I had orthotics, splints, injections - everything - over a 12 month period. Nothing helped and I woke one day wanting to cut off my foot (seriously, that is what I told my wife).
After changing from a PPO to Kaiser, I once again visited the Podiatrist. The doctor immediately said, "If you've tried other remedies, then you need surgery." I had the surgery two weeks later, and was walking with a padded covering the next day. The difference almost brought tears to my eyes.
I know of two others (also runners) who have had MN and the only remedy was surgery. The podiatrists I fired were all unable to perform the surgery, so they tried to offer every remedy under the sun except the only one that would help. Makes me angry even typing this.
I now have MN in my other foot (presumably years of running and years of marching are taking their toll). I see my doctor next week and I am quite certain that he will go back and pull the nerve. IT IS THE ONLY TRUE REMEDY IF YOU ARE IN PAIN.
Dr. Blake - saying that only 5% require surgery simply cannot be true and is certainly misleading to the patients seeking comfort in a very painful foot. I fear that they will follow the guidance and try to seek comfort with other treatments for at least one year (as you suggest) like I did. For the third of sufferers who have the pain in their foot, especially at the 8-10 on the pain scale, they will not be cured with orthotics, therapy, injections, etc. Surgery is their only cure.
Dr Blake's Response:
Thank you so very much for your heartfelt comment. Most of my patients who have surgery for Morton's Neuroma feel the same way. When you need surgery for Morton's Neuroma, you should have it. This does not however mean that conservative treatments should not be tried before surgery is undertaken.
There is typically a 3 month window of time after the patient first presents with MN pain that 2 things happen: A) an attempt at conservative treatment is initiated, and B) MRI documentation along with an evaluation of other causes of nerve pain. If by the end of the first 3 months, the conservative treatment is not working well, the MRI documents a MN, and other forms of nerve pain (like low back referred pain) are ruled out, surgery is recommended.
The gray areas come from patients where the pain is, or is becoming, manageable, the MRIs are inconclusive, and there is some suggestion of low back involvement.
So, I am very happy for you. I am biased to avoid surgery when possible, and that bias does come across strongly. I always feel bad when the patient and I work hard together to avoid surgery, but in the end surgery is needed. But, my patients know that if conservative treatment fails, surgery is our last resort option. How does conservative treatment fail? One way is that the pain level is not managed in the 0-2 range (Good Pain). During the first few months, while conservative treatment is being explored, it is imperative to do whatever to get the pain under control. This is more true for nerves than any other structure.
Below is the blog post that the patient above was responding to.
Morton's Neuromas: Which Shots to Get?

Morton's Neuromas are inflamed swollen nerves in the front of your foot, usually found between the third and fourth metatarsals(as seen in the above MRI), and sometimes between the second and third metatarsals, and sometimes between both. You count the metatarsals from the big toe #1 to the pinky (baby) toe #5. The symptoms from these inflamed nerves are nerve symptoms: burning, tingling, numbness, electrical, radiating, buzzing, sharp, and/or feeling like a rolled up sock. They are abnormal sensations, also called dyskinesias (just to show you how smart I am). But, this pain may be not be from the foot at all. Nerve pain in the foot can originate from nerve irritation at the ankle, knee, hip, or low back. Nerve pain in the foot can also be systemic (from the body) called peripheral neuropathy. So, it can be very challenging to diagnosis the source of pain in many patients, and thus treat it properly. Any workup for nerve symptoms in the foot should look for possible causes other than the foot.

Photo shows typical problem between 3rd and 4th metatarsals.
One of the mainstay treatments of Morton's Neuromas involves injections. There are three common shots, and other combinations of medications used in injection form. First of all, there is the diagnostic injection of local anesthesia (like novacaine) to see if injecting the nerve gives complete pain relief. It sometimes proves that the nerve the doctor thought was the problem really is not the problem. These local anesthetic injections should be given with medications that last around 5 hours (commonly Sensorcaine, Marcaine, or Bupivacaine) so that the patient can be 100% sure of the relief attained--100%, 80%, 50%, 30%, or 0%. I am a big believer in this method of identifying the right nerve, if it is a nerve at all, since you only inject the nerve and not the tendons, ligaments, joints, etc. Sometimes, even though you are giving an injection which should last 5 hours, since you are blocking the pain cycle, the relief can be much, much longer. Many doctors will give these injections once or twice a week until the severe pain cycle is completely broken down and the symptoms greatly minimized.
The second most common type of injection involves cortisone. No one knows for sure how much should be given, since that varies from person to person and body part to body part, but I have lived by the rule of no more than 5 shots per year. I can count on one hand how many patients have needed more than 3 per year, so 4 or 5 shots is unusual, but sometimes necessary. Each one of my cortisone shots is 10mg of long acting steriod.Long acting means that some of the medication is still working for 9 months.As the crystal dissolves, there is slowly less cortisone working on a daily basis. Cortisone can allow healing to occur since it removes swelling. Swelling is our enemy. Swelling cuts off the normal circulation to an area inhibiting healing. So it it more than just a bandaid or temporary fix--it can fix the problem!! I find no use for short acting cortisone. It only lasts for 3 days or so. So what? If you think the patient needs cortisone, use the good stuff. I once had a patient come in for surgical consultation after she failed to improve with 10 cortisone injections over a 6 month period. Surgery had been recommended, and it was a simple appointment to verify that this was appropriate. When we found out what the doctor had used in each injection, I was dumbfounded. He was using long acting cortisone, but in a homeopathic dose of 0.1mg per shot. If you do the math, you would realize that it would take him 100 shots to equal the dosage of one of my shots. Oh my!!??!!
Why am I discussing dose? Because you should know if you are getting a foot or ankle shot, if it is long or short-acting cortisone, and how much? The 5 injection recommendation per year is based on actually getting 50 mg of long acting cortisone in one area. It does not mean that you can not get the same amount in another area of your foot. One smart patient, with one smart doctor, helped me understand that a local cortisone shot can affect the entire body since small amounts do get absorbed into the body. I call this Dorothy's Rule, after one of my patients, that a patient should not get more than 1 shot of long acting cortisone per month for their entire body. I like this rule since cortisone does affect us in many ways. This applies to patients whom are getting cortisone shots for their foot, and at the same time for their knee, shoulder, etc.
When giving cortisone shots the doctor should stay away from the skin, burying the injection as deep as possible, and avoid tendons if possible. Cortisone near a tendon can weaken it, and cause tearing, as it can thin the skin. The skin usually gradually gets healthy, but can take 9 months or longer, and can not tolerate further shots until this time. Cortisone is normally mixed with the long acting local anesthetics to get 5 hours of post shot pain relief. If the patient does not feel any relief after the shot, the shot missed the painful spot. After cortisone, patients are told no running or jumping for 2 weeks (another reason athletes hate cortisone shots). The patients are told to check pain relief in the first 5 hours, at a week, and at the 2 week followup. If the 10mg is not enough (with the goal 80% reduction in pain), a second shot is given and the two weeks starts over again. During these shots, I do not have the patient go to physical therapy, but they can cross train with non jumping and running activities. With many activities like cycling, they have to assess if it has a negative impact on them. During these shots, the patients are told to ice the area 3 times daily. At each two week interval, if the patient seems to be at the 80% level (familiarize yourself with a pain chart and read Chapter 2 on the Magical 80% Rule), activity is gradually returned. Hopefully, the doctor and patient have learned what to avoid, what to wear in the shoes, how to tape, etc, to minimize the re-irritation during the return to activity program. Any cortisone shot after the first shot in the 9 month window of time is considered a booster shot.
The third most common type of shot is to destroy the nerve with alcohol. I mix long acting local anesthetic with 100% concentrated denatured alcohol to achieve a 6% alcohol solution. Then 1 ml of this solution is injected straight into the nerve in one spot (where you believe the nerve is the thinnest--typically just before/proximal to the neuroma). Topical cold spray is used to anesthetize the skin, so 100% of the medicine is deposited into the nerve. These injections are given in series of 5, each one 7 to 10 days apart. 50% of patients get excellent results, 20% good (some improvement) and 30% none. After each series, 1 month is recommended to rest the soft tissue. If the patient noted no response from the first series, a second series is not normally recommended. Of the patients alcohol helps 20% or so need only 1 series of 5 injections to feel 80% better, 70% need 2 series, and 10% need 3 series. I know this is a lot of numbers, but I love numbers, and this is my stats so I am sticking to them!! As with the photo at the start of this article, the bigger the neuroma on MRI, the less likely the alcohol shots will work. But, the art of all this is deciding who has a chance. If it was my foot, I would go through the alcohol series to achieve the 80%, and if 80% were not achieved, I would get sporadic cortisone shots, get great orthotic devices that take pressure off the area, ice my foot 2 to 3 times daily, and do the other things recommended. You can also give the cortisone shots while doing the alcohol shots if there is an unexpected flare-up.
Morton's Neuromas: Advice for When Pain Becomes Chronic
Dr. Blake,
I have read your blog on Morton's Neuroma. I have been suffering with the affliction for over two years and it literally almost killed me.
To start, I'm 52, male, in good health otherwise. Non-drinker, non-smoker. My foot pain started in November of 2007 rather insidiously. In January of 2008, I visited a podiatrist who diagnosed the condition and gave me a cortisone shot.
This shot ended up causing me tremendous pain for over two months. I was ready to cut my foot off it hurt so much.
During this time I researched the condition and learned about all the pitfalls of surgical intervention for the condition. After much research, (MRI, visiting several different physicians) I learned that my condition is caused by foot mechanics. I have what has been described as a hypermobile first ray which directs my weight to the center of my forefoot during walking.
I have one neuroma between 3 and 4 on my left foot. Two on my right foot, one between two and three, one between 3 and 4.
I have spent literally thousands of dollars on shoes, orthotics, two rounds of cryogenic neuroblation, one by a doctor in Tampa (Dec 2008), a second by a doctor in Phoenix, (Dec. 2009). My symptoms have lessened but I can not stand still for more than 5 minutes without pain, and cannot work standing all day without ending up in a lot of pain.
The Cryo really helped my left foot and the neuroma between 2 and 3 on my right foot, but, the neuroma between 3 and 4 on my right foot has really started to bother me again.
By the way, when I said that this condition almost killed me I meant it. I had been taking Celebrex to help manage the pain for over 1 year. (200 - 400 mg per day depending on pain started in 12/08 after the first cryo). In July of this year I was put in the hospital with a bleeding ulcer. This was an expensive ($60,000) event, along with the 10 day hospital stay. My gastroenterologist feels that the ulcer was from the NSAIDS, as I do not have an H-Pylori infection.
I need to get this problem resolved. I am trying one last pedorthist for a set of orthotics and shoes that help with my gait. I am considering either one more Cryo attempt, or getting some guts up and going for the surgery.
With the mechanical issues that come with my inherited feet (one doctor told me that I just had bad genetic luck ) I wonder what is my best course of action. I prefer the cryogenic neuroablation over the alcohol shots but I am wondering if it is time for surgery.
In your experience how common are complications from the surgery, stump neuromas, complex regional pain syndrome, etc. Would you try something else ? The pain from this condition is affecting my life not only at work, but in my relationship with my family and my overall general health as I can't walk, bike or exercise any more.
The possibility of the surgery actually making the pain worse scares the day lights out of me because I don't know if I could take it.
Your blog (drblakeshealingsole) is very informative and it sounds like your approach is very conservative. You seem to be a talented and compassionate individual. I would appreciate any thoughts you have in this matter.
Thank you for your time.
Brian
Brian, Thanks for the compliments and email. There is so much to discuss from your email, and I thank you for allowing me to answer in my blog post.
One of the main reasons I would not go to surgery now, if you have told us everything, is that you need more work up for the source of the nerve pain. I do not think you can ever be sure that nerve pain has a simple source, like a fallen arch, or a hypermobile first ray. But, great orthotics can help you immensely and must be sought after, as long as you are in shoes wide enough to accommodate them. There are so many factors when dealing with orthotics and nerve pain that it can take quite awhile to recognize them all and address them all. They include the amount and placement of the metatarsal arch, the flexibility or stiffness of the material around the metatarsals, the accommodation, and exact placement of for the painful spot, the heel pitch forward, etc, to name a few. Have you been happy with the orthotic people you have gone to, are they analyzing many of these factors? The orthotic support therefore must be as ideal as possible before you venture into surgery, and it may eliminate your need for it. I guess what I am trying to tell you is not to set some arbitrary number on how many orthotics you get before surgery, but to keep trying until at least you feel the guy making them is doing the best for you.
One of the key aspects of your condition right now is to regain foot strength.Golden Rule of Foot: For every day you are in pain, it takes another day to get the lost strength back. That is one reason you are on this slow course. Loss of foot strength definitely is allowing the metatarsals to collapse onto the nerves increasing the nerve irritation. You need a skilled physical therapist to triple the strength in your feet over the next year, but the exercises you do can not increase the nerve pain. Sometimes this is easy, and sometimes this is a difficult task. But, it is extremely important however.
One question all patients with neuromas must ask is why do my neuromas hurt, when some neuromas do not. I have done an MRI on many patient's feet and found non-painful neuromas, at least the patients say that they have never hurt. I have had patients who come in with neuroma pain for 2 weeks, and when we MRI them, they have some of the biggest neuromas west of the mississippi (I live in California). Why did they just start to hurt? The neuromas had probably been around for years. The word Neuroma denotes some permanence, a thick scarred swollen tumor. But, inflammation of the peripheral nerves called neuritis, does not show up on MRI, and can hurt just as bad, and require just as much treatment. I think neuritis responds better to alcohol shots, but this is another general rule that may not apply to you. So you need to make sure that your neuromas hurt by themselves and not complicated by tarsal tunnel syndrome, peripheral neuropathy, low back radiculopathy, and other sources of nerve pain. You definitely need a neurologist or physiatrist involved. Nerve Conduction Studies can be very helpful for tarsal tunnel and low back involvement. Nerve biopsy, and some lab work, is standard for peripheral neuritis. So, the source of the pain must be identified better.
I am not sure why cortisone shots help 99% of patients and aggravate 1%. And when it aggravates, called steroid flares, these patients really hurt for a long time, and they never want another shot again. Don't blame them. Sorry it happened to you.
I have no experience with cryoablation, but it sounds like it helped 2 of the 3 areas. Sounds like you respond well to it, what have they told you about it not working if you try it again. Was it very painful? What is the downside in your mind? Please answer any of these questions in the comment section of this post.
I am a little unclear if you still have pain in one or both feet. Could you let us know when you have pain during the day, and at what level on the pain scale of 0 to 10? Have you tried a removable cast, with or without an orthotic, on the worse side and does that take care of 100% of your pain when you are wearing it? Have you tried athletic shoes, hiking shoes, clogs, or sandals, and do any of these shoe gear changes help you at all? Golden Rule of Foot: Try alternating shoe gear throughout the day to vary the stresses on an injured area.

Since all of the nerves involved have been poked on repeatedly, there can easily be a two year healing course that you are presently on, where the pain will gradually get better. I prefer you keep working on the orthotics, get a pain specialist (neurologist or physiatrist) on board for evaluation and treatment recommendations, find ways of being more active ( there has to be a way you can ride your bike without pain) for

strength/cardiovascular/emotional health, use Neuro-Eze three times daily or a prescription compound, consider alcohol series for the stubborn nerve, discover what shoe factors make you hurt more and less, do contrast bathes or warm soaks twice daily, place a removable cast on for part of the day if that helps, use Neurontin or Lyrica to desensitize the nerves for a 6 month trial (must start real low dose to get used to it), play with digital splints and taping if the orthotics reach a limit of what they can do, and consider at least another office visit where the doctor injects your nerves with local anesthetic(diagnostic test) and eliminates your pain for 5 hours completely. I hope this refocuses you and I will be following your comments. There is so much to do prior to considering surgery that I will save the surgical questions indefinitely.
No comments:
Post a Comment
Thank you very much for leaving a comment. Due to my time restraints, some comments may not be answered.I will answer questions that I feel will help the community as a whole.. I can only answer medical questions in a general form. No specific answers can be given. Please consult a podiatrist, therapist, orthopedist, or sports medicine physician in your area for specific questions.