Welcome to my Google Document that I shared with my Podiatry Students at the California School of Podiatric Medicine Samuel Merritt University Oakland, California. This was my first Zoom teaching, so I over prepared, and dropped everything else I was doing last week, but I think it went well. I will be putting the answers to questions on this on request of student doctor Diksha Mohapatra by April 17th, 2020. The videos are great to watch if you want to learn about gait evaluation. Rich
Biomechanics Workshop Outline (4/10/2020 1-3 pm)
Biomechanics Workshop Outline (4/10/2020 1-3 pm)
- Introduction of Students and Dr. Rich Blake
- Allison Ma
- Amy Lau
- Andrew Rasiah
- Diksha Mohapatra
- Maksim Rukhalskiy
- Shane Hall
- Usman Khokhar
- Yona Mizrahi
2 Classes from Dr. Rich Blake Gait Evaluation 4/10/2020
Orthotic Devices on 4/24/2020
(we will start next session with the discussion of the assignment below on Golden Rules)
I hope to teach you that Gait Evaluation is much more than pronation or supination of the foot. Look at the whole body. We use gait evaluation as a clue to find out what is wrong with a patient, and how to help them.
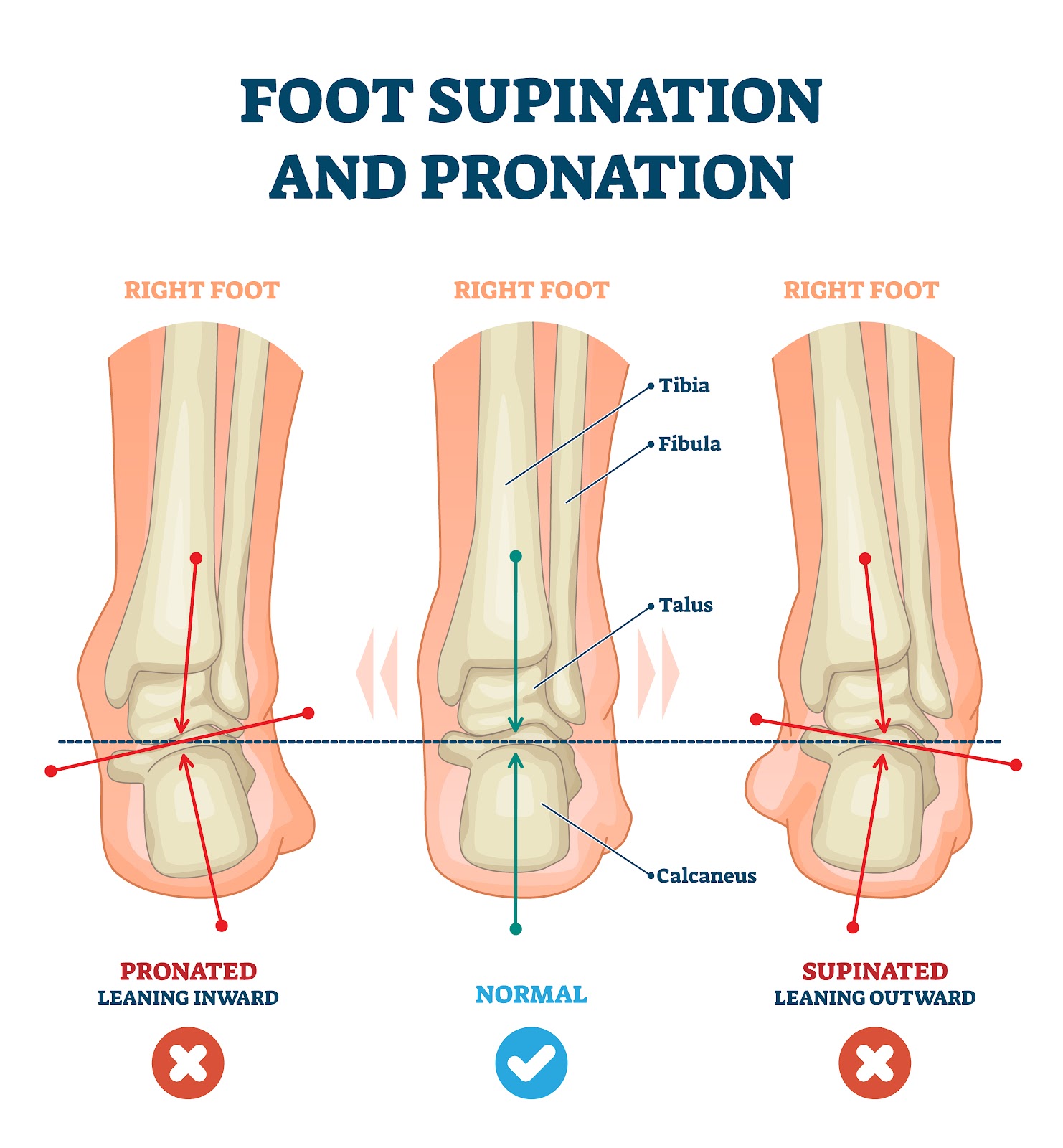
Right Foot
Some of your patients will like this video, so you should know how to treat them and we will go over orthotic devices next session.
I want to introduce my blog www.drblakeshealingsole.com which will have a lot of info. My YouTube channel is also entitled drblakeshealingsole
Maksim: What are the 5 common mechanical problems picked up in gait?
Shane: Give me an example of a problem related to a tight muscle?
Usman: Give me an example of pain related to a short leg syndrome?
Yona: What would be the general treatment categories of these 5 mechanical problems?
Allison: What are the 2 separate parts of gait called?
Amy: What are the 5 components of stance phase?
Andrew: What are the 3 components of the swing phase?
Diksha: With what you know of the contact phase as the ankle is plantar flexing, what is the heel doing in the frontal plane and the knee doing in the transverse plane?
Maksim: How does the patient prevent foot slap gait with drop foot?
The common findings in gait that you as a podiatrist will see in regular practice is less pathological and more subtle, but still very important. Looking to see how to help each patient mechanically.
- Ability or Inability to Walk (First and Foremost)
- Structural deformities like pes planus, pes cavus, bow legs, knock knees, genu valgum, etc.
- Signs of Asymmetry
- Signs of Pronation
- Signs of Supination
- Signs of Limb Length Discrepancy
- Signs of Tight Muscles/Tendons
- Signs of Weak Muscles
- Signs of Poor Shock Absorption
These are all problems that we can make mechanical changes to help
Maksim: What would be a sign of pronation?
Shane: What would be a sign of supination?
Usman: What would be a sign of short leg syndrome?
Yona: What would be a sign of tight muscles?
Allison: What would be a sign of weak external hip rotators?
Amy: What would be a sign of weak achilles tendons?
Andrew: What would be a sign of weak peroneal tendons?
Diksha: What would be a sign or weak posterior tibial tendon?
Maksim: What would sign of poor shock absorption?
Below is a video with a more podiatric approach with less emphasis on the aspects of gait, and more on what can cause injury that we can help.
Maksim: What does good arm swing correlate to in the lower extremity?
Shane: If excessive supination was found in the left foot, and it correlated to some symptom like peroneal strain, what could be done about it?
Usman: What is significant about knee internal rotation at heel contact?
Yona: If you saw excessive internal knee rotation at heel contact, what muscle group could be weak?
Here is a video on over pronation?
Amy: What are 3 foot problems caused by overpronation?
Allison: What are 2 knee problems caused by overpronation?
Andrew: What muscles would you have a PT strength with overpronation syndrome?
Diksha: Which types of shoes help with overpronation?
Here is a video on over supination?
Maksim: What are 4 problems caused by over supination at the foot?
Shane: What are 2 knee problems caused by over supination at the knee?
Usman: How does over supination cause joint pain and stress fractures?
Yona: What are 2 muscles/tendons to strengthen with over supination?
Here is a video on limb dominance?
Shane: What are the 4 main gait findings that may suggest short leg syndrome?
Where does gait fit into our General Approach to Injuries and Pain Syndromes?
14 Step Approach to a Injury or Pain in Office Visit
These are the common steps in a general biomechanical approach for the first several visits dealing with a new patient or new problem:
- History of the injury and the patient’s reason why they were injured.
- Gait evaluation of walking (running is crucial if their activity requires running) to decide on gait patterns and if the patient’s complaint matches)
- Physical examination of the injured part (begin to separate the 3 sources of pain: mechanical, inflammatory, and neuropathic)
- Physical examination of possible biomechanics involved
- Is there biomechanical asymmetry?
- Tentative working diagnosis made
- Common Differential Diagnosis: common not rare
- Occam’s Razor and the Rule of 3 for initial treatment help
- What Phase of Rehabilitation is the patient in at this visit?
- Should we do Imaging at this point?
- First Decision: What do I have to do to get the pain consistently between 0-2? This is the real reason that the patient has to be put into Phase 1 of Rehabilitation where PRICE rules. The 0-2 pain level realm is where injuries can heal.
- Second Decision: How Much Inflammation needs to be Addressed?
- Third Decision: Is there any neurological component that should be treated?
- Fourth Decision: What mechanical changes can I make in the first few visits that may help the pain relief, better biomechanics, and cause reversal?
Since I can never get enough on gait evaluation, here is another video.
Amy: How many steps equals a stride?
Allison: What happens first, heel lift of the right or heel contact of the left?
Andrew: Why is it important to watch both sides?
Diksha: Did the patient have tibial varum or valgum?
- Common Gait Findings (Summary)
Gait Evaluation Checklist (circle findings)
- Head Tilt (Straight, Lean Right, Lean Left)
- Shoulder Drop
- Asymmetrical Arm Swing
- Dominance to One Side
- Trunk Mobility (Limited, Normal, Excessive)
- Hip Hike (Right or Left)
- Belt Line (Higher Right or Left)
- Hip Rotation (limited, normal, excessive)
- Excessive Shock (Right or Left or Both)
- Limited Knee Rotation(Right—straight vs external, Left—straight vs external)
- Excessive Internal Knee Rotation (Right or Left or Both)
- Heel Motion at Heel Contact (Right—eversion, none, inversion, Left—eversion, none, inversion)
- Symmetry of Arch Collapse (Right more vs Left more)
- Digital Clawing (Right or Left or Both)
- Angle of Gait (Right—internal, straight, external, Left—internal, straight, external)
- Other Structural Variations: Pes Cavus, Pes Planus, Tibial Varum, Genu Valgum, etc
- Correlation to Symptoms: _____________________________________________________________________________________________________________________________________________________________________________________________
- Other Observations: ______________________________________________________________________________________________________________________________________________
Allison Question #1: In assessing gait in an adult, the finding of a head tilt to the right suggests which leg is possibly longer?
Amy Question #2: When you observe a patient walk, and you note that their right shoulder is lower, what should you ask them and where should you next observe?
Andrew Question #3: Asymmetrical shoulder motion is typically reflected in asymmetrical arm motion. If a patient has a sore right knee, what is the normal arm swing variance seen, and how can that cause neck pain?
Diksha Question #4: As we continue to evaluate gait, what are the signs now that the patient has a possible treatable limb length discrepancy?
Maksim Question #5: How does the correction of 12 degrees of forefoot valgus deformity help with back pain from muscular tension?
Shane Question #6: What does it mean for you to observe Hip Hike?
Usman Question #7: Watching the beltline of a patient as they watch back and forth in your clinic typically gives you 3 observations that you may be able to treat. These observations are:
Yona Question #8: The normal knee motion is a reflection of hip motion. What would it mean if the knee started central or straight, and externally rotated to an external position during the contact phase?
Allison Question #9: How can a patient maximally pronated in gait due to genu valgum and weak posterior tibial tendons be a poor shock absorber and present with knee pain?
Amy Question #10: A patient complains of lateral foot pain recently. They have observed that their foot was out toed more in the last several years. They have some back pain also. What is the possible diagnosis?
Andrew Question #11: Excessive internal rotation of the knee is a common gait finding. What 3 areas of treatment should be addressed?
Diksha Question #12: As we learn to watch gait, what motions are found with the motion of heel eversion and heel inversion?
Maksim Question #13: When a patient with pes cavus walks towards you, you do not observe any flattening of the medial arch on the right foot, but marked arch collapse on the left side. We understand that there are pronatory forces occurring on the left, but what could be happening on the right?
Shane Question #14: In gait we may observe that the toes tend to claw. This can be bilateral or occasionally unilateral. What are 2 common reasons that weak achilles tendons can cause this? What is the acid test for achilles strength?
Usman Question #15: As we watch a patient walk, one of the last observations will be the angle of gait. It is really important for children to know what the reasons are for the internal or external angles because of our abilities to cast or brace young children to improve this transverse plane issue. If you observed in gait that the knee was straight, but the foot 30-40 degrees externally rotated, what are several common causes?
Yona Question #16: The general rule used in shoe stores is that pes cavus feet supinate or underpronate. What percentage of pes cavus feet supinate?
Here is a video from the running shoe Company
Shane: What are the 2 types of overpronators they described?
Yona: What does the term Underpronation mean?
So, here is a summary of the gait findings I find daily in my patients associated with the common mechanical syndromes that I can make correlations to their symptoms and then treat mechanically.
Common Signs of Short Leg Syndrome
- Limb Dominance where the patient spends more of their time over one side
- Asymmetrical arm swing (long leg can have the arm closer to the body)
- Shoulder drop is usually to the long side (when compensated with the spine)
- Head tilt is usually to the short side (also when compensated with the spine)
- More pronation or more supination on one side
- Belt height is angled up towards one side
Amy: Which statements are false in leg length discrepancies?
- The typical limb dominance is to the long leg
- A true shoulder drop finding has lower fingers on that side
- The more pronated side is the shorter side
- The Standing AP Pelvis x-ray without lifts is the most important x-ray
Common Signs of Excessive Pronation
- Internal rotation at the knees is excessive
- The medial prominence of the ankle
- Digital clawing in midstance
- Abductory twist seen in propulsion
- Heel eversion is sometimes seen
- Arch collapse is noticeable as the patient walks toward you
Allison: What would not be considered abnormal pronation?
- Pronation after heel contact too rapid
- Pronation after heel contact too prolonged
- Pronation after heel contact excessively internally rotating the knee
- Pronation to heel vertical in 10 degrees of tibial varum
- Pronation to a 2 degree everted position before the midstance phase
Common Signs of Excessive Supination
- Lateral shift of the body weight following heel contact
- Heel Inversion at heel contact is sometimes seen
- No patellar internal rotation at heel contact
- Gait sometimes appears very rigid
- Sometimes shock wave up calf and thigh seen
- Lack of arch collapse at contact
Andrew: Which of these problems is not related to overuse of the peroneal tendons trying to decelerate abnormal heel contact supination?
- Peroneal Tendonitis
- Fibular Stress Fractures
- Inversion Ankle Sprains
- Tibial Stress Fractures
Common Signs of Poor Shock Absorption
- A loud sound of heel strike
- Shuttering of the muscles (especially calf and thigh) following heel contact
- The rigid appearance of lower extremity
- Excessive subtalar joint supination at heel contact
- No Subtalar Joint Motion Observed
Diksha: A patient with lower back pain and limb dominance noted on gait evaluation may be caused by what problem?
- Limb Length Discrepancy
- Excessive Unilateral Pronation
- Excessive Unilateral Supination
- Poor Shock Absorption
- More than one cause
Common Signs of Equinus
- Early Heel Off
- Bouncy Gait with heels barely touching
- Genu Recurvatum with excessive straightening of the knee
- Excessive pronation typically with out-toeing gait
- The collapse of the midfoot after heel off
Maksim: Severe equinus forces can cause severe pronatory forces on the foot needing to adapt. Discuss the concept of a “double heel lift” occasionally seen.
Common Signs of Typical Severely Weak Muscles
- Medial arch collapse with weak posterior tibial tendon
- Lack of heel lift with weak achilles complex
- Excessive internal patellar rotation with weak external hip rotators
- Lean to one side with weak hip abductors
- Contact Phase Lateral Instability with weak peroneal tendons
Yona: Posterior Tibial Tendon Dysfunction can be treated conservatively even in some Stage 3 patients. What are 3 major functions of the posterior tibial tendon that may need help in the rehabilitation, and the 2 functions helped with corrective custom made orthotic devices?
For next class, I am assigning this presentation on the 20 Golden Rules of Athletic Rehabilitation. Please be ready to discuss the ones assigned to you.
Allison 1, 9, 17
Amy 2, 10, 18
Andrew 3, 11, 19
Diksha 4, 12, 20
Maksim 5, 13
Shane 6, 14
Usman 7, 15
Yona 8, 16
This is the assignment for the next 2 weeks. You need to email Dr. Blake your answers and please do not all wait until before the next class!! LOL
Examples of Gait Findings and Treatment Options
Example #1
A runner presents after developing left knee pain on a long training run preparing for the San Francisco Marathon that was to be two months later. Gait evaluation walking revealed a dominance (or body shift) to the left side suggesting at least more weight bearing on the injured left side and perhaps a short leg syndrome. This dominance to the injured side is also significant due to the fact it is opposite of mere favoring to take the load off the injury. The left knee had more internal rotation at heel contact on the side of the runner’s knee complaint. The heel was actually inverting at heel contact (opposite direction of the knee internal rotation). The patient was then asked to run up and down a long hallway with the running shoes that they brought into the office. It was a brand new pair, as they had purchased in hopes it would clear the knee problem. I asked the patient to bring in the pair she was wearing when she hurt the knee.
Remember the Rule of 3 in evaluating these overuse injuries (from Chapters 1 and 2). Any injury, where the tissue is so overstressed that it begins to complain, typically has at least 3 causes (yes, you do not need to stop at three). This is why one patient with overuse, or overpronation, or wears inadequate shoes, can develop knee pain, another shin splints, another foot pain, and so on. It is a fun investigation and of course, should be started on the first visit on the new problem or new injury. In this case, the left knee pain was being stressed by:
- An inadequate training program (she was up to 15 miles only two months after starting running)
- A dominance to the left probably placing 20% or more weight on the left side (later found that the left side was the long leg of a ¼ inch)
- Excessive internal patellar rotation caused by very hip external rotators (yet, quickly improved with an appropriate strengthening program)
- Unstable athletic shoes with poor support and cushion (discovered at the second visit)
- I also think that when the knee is going in one direction (internal) and the foot going in the opposite direction (external) there must be terrible unnatural twisting motions whose stress must be taken up somewhere
- Other components discovered were weak quadriceps, tight hamstrings, and low Vitamin D (not sure if there was a relationship here).
- Also, she lived on the bottom of a huge hill in San Francisco, and her running loop always had her run the last mile down hills when her legs were the most tired.
So, gait evaluation pointed the way to several key components that were easy to correct in the long run. This particular patient would go on to run several marathons over the next few years with strong external hip rotators and quads, a good training problem, and Brooks Glycerin Shoes for her supination. She knows she has one leg longer, and someday that may be addressed. She reversed the Vitamin D deficiency, and if she breaks anything a bone density will be ordered. Her primary care physician thought at 32 years old, and no history of fractures, a bone density scan was not called for in this case. It took 6 months to get the external hip rotators strong, and initially, the therapist was not isolating the external hip rotators enough and not stretching the tight upper part of the medial hamstrings. When you imagine that the average runner quits running within a year, runners really appreciate this type of approach towards wellness and long-term prevention. This example also points to the fact that you do not need to always correct everything at first, but I love my patients to definitely know what is going on.
All Students: Utilizing the Rule of 3 for gradual sesamoid pain developing in a hiker, what are some common causes in an overuse situation? Email me answer at rlb756@gmail.com
Example #2
This 76 year old noticed pain in the lateral side of her left foot 6 months before the initial office visit. The problem has been getting worse and more limiting. She also noted some flattening of her left foot in the last few months. Gait evaluation showed markedly more pronation on the left foot compared to the uninvolved right foot, with heel valgus only seen on the left side. She noted swelling medially, but the pain was only lateral. We are obviously dealing with posterior tibial tendon dysfunction but it is not the usual location of pain. By again using our Rule of 3, the examination found (more than 3 or sure):
- Very weak posterior tibial tendon
- Very weak Achilles’ tendon with overstretched length
- 12-degree heel valgus resting position measured, and 3 degrees valgus or everted on the right side
- The tendency to wear heels or flats with no support
- 30-year-old left ankle sprain with questionable rehabilitation
- Not an ounce of athletic sense or body awareness when discussing rehabilitation with her
- Overweight
- Inactive her whole life (busy professional until retirement)
Gait evaluation pointed to the pronation problem left greater than right. The significant heel valgus would have been missed without gait analysis with the asymmetry very important. She had been dealing with weak muscles for a long time, but the heel valgus was causing lateral ankle impingement (between the calcaneus and the fibula). MRI showed some irregularities in the tendon but no tear. She really had pronation pain, not posterior tibial tendon dysfunction pain. She knew she had neglected her health, but fought diligently to take stress off the lateral ankle and was quite simple to treat in some ways. The 6 things that turned her symptoms around:
- Stable shoes and ⅜ inch varus wedge (¼ inch for the uninvolved right side)
- Joined Weight Watchers and lost 22 in 3 months
- Began a one year program of posterior tibial, Achilles, single leg balancing, external hip rotator strengthening (probably had doubled her initial strength in the first 2 months)
- Icing 3 times daily for anti-inflammatory
- Leukotape with coverlet to prevent heel eversion (helped the varus wedge)
- Several dressier flats, that could not hold the varus wedge internally, had ¼ inch varus outsole wedging applied full length by a local cobbler on the left and ⅛ inch on the right side.
I am not mentioning the functional orthotics she received in the modalities that turned her around because she was so much better months before they were dispensed, and I actually never saw her wear them except at the orthotic dispense visit 4 months into our journey together. She was given highly corrective orthotics for the left (35 degrees, and 20 degrees for the lesser pronated right foot). Both athletic and dress versions were made, and because Medicare does not pay for them, she self-paid for this and only this part of the treatments. Chapter 13 on custom orthotic devices will go into the rationale of how many degrees of correction to order. She said they will be used in some hiking boots, but she always came into the visits in dress shoes with the outer sole with the varus wedge.
I said that she was easy to treat in some ways because the real reason I remember her is that the first podiatrist she saw immediately used the “S” word. This podiatrist did watch her walk, and saw the pronation. She was immediately placed into the adult acquired flat foot reconstruction category, and without MRI or a lot of thought, had scheduled her for flat foot reconstruction with the breaking of the heel bone, fusion of some joint, and repairing tendons (patient’s description to me). She only saw me because a friend had seen me and told her to at least get another opinion. I only saw her five times, about one month apart. The first visit was for an hour and we talked about the surgery for 45 minutes of the visit, the next visits were 30 minutes each and each visit we talked about the surgery a little less and less. The last visit, she was completely out of pain, walking 30 minutes daily, no discussion of surgery until as she left the office she turned around and said: “how will I know when I need surgery?” The power of a word. I saw her one year later for follow up and an ingrown toenail, she looked 20 years younger, 37 lb weight loss overall, exercising regularly and did not say the “S” word.
All Students: Research to find out how much inversion I would put into this foot using the Inverted Orthotic Device initially. Email answer rlb756@gmail.com
No comments:
Post a Comment
Thank you very much for leaving a comment. Due to my time restraints, some comments may not be answered.I will answer questions that I feel will help the community as a whole.. I can only answer medical questions in a general form. No specific answers can be given. Please consult a podiatrist, therapist, orthopedist, or sports medicine physician in your area for specific questions.