Accessory Navicular Syndrome
The accessory navicular would be next to and to the left of the navicular. It can be so big that it looks like a second ankle bone.
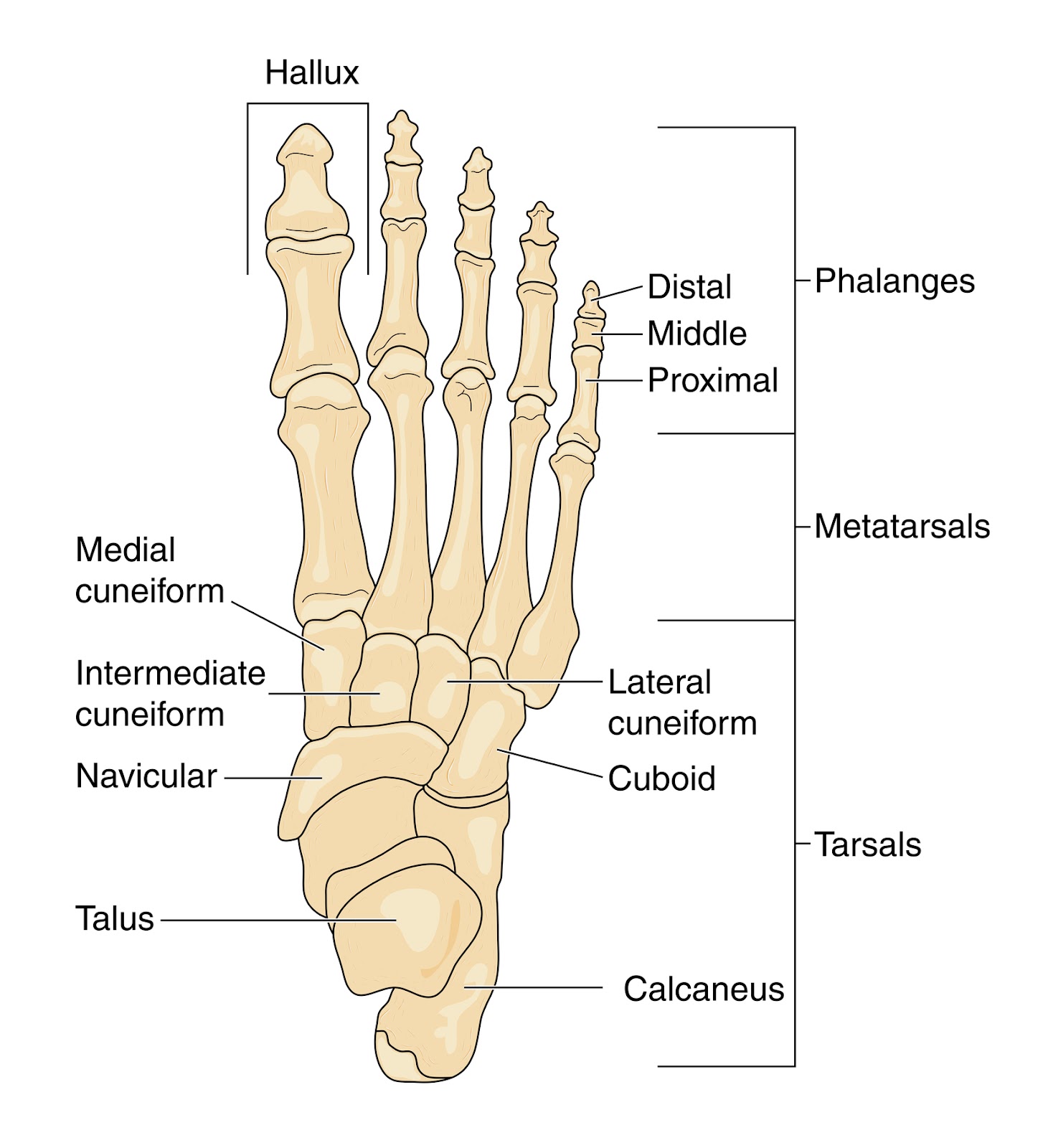
Here I am separating posterior tibial problems from a unique problem which occurs where the posterior tibial tendon attaches into the navicular. From that point, the navicular spreads under the midfoot supporting the arch with multiple attachments. When you have an accessory bone where the posterior tibial tendon attaches (around 3% of the population) much of the force is lost that supports the arch. The normal tendon attaches into the extra bone, which has little to no arch support function, instead of where it should go. A syndrome of pain, arch collapse, and mystery can occur. The mystery is that at times the accessory bone needs to be removed, but most of the time you can co-exist with it (95% of the time). Even in the 5% that need surgery, it takes a lot of time trying to avoid surgery to find those that really need it.
The top 10 treatments for accessory navicular syndrome:
1. An MRI is very important to discover what the source of pain actually is: stress fracture, joint inflammation, or tendinitis. There is a joint between the navicular and its accessory bone.
2. Use Kinesio Taping or supportthefoot.com tape or classic low dye taping techniques intially 24/7 and then for extended activities.
3. Ice pack the sore area 10-15 minutes 3 times daily.
4. Go into a removable boot (such as an Anklizer) for 2-3 months if needed to calm the foot down.
5. Strengthen the posterior tibial tendon starting initially with active range of motion like ankle circles.
6. Check out the Aircast Airlift PTTD brace to see if it is helpful for you and can get you out of the boot faster.
7. Custom foot orthotics are a must for a 2 year period. They must produce a good force against the navicular, but it may take time finding the right orthotic guy/gal.
8. You can use Sole OTC orthotic devices with medial longitudinal Hapads initially until a good protective orthotic device is made.
9. Create a pain free environment as soon as possible (level 0-2).
10. If the MRI shows bone reaction (edema), order a bone stimulator as soon as possible to start strengthening the bone.
Email Correspondance:

Dear Dr. Blake, I was wondering if you would be able to clarify some information to help us make some smart treatment decisions. My 13 year old daughter is a high level soccer player. She started to complain of pain in her foot last spring during the time she played soccer and ran track. She also played in 14 games of soccer without ever coming out. A significant increase in activity. The pain was located on a bump that has been recently identified as an accessory navicular. She was first treated with rest and 4 weeks of physical therapy and orthotics. After returning to sport the pain returned but was slightly higher above the ankle. MRI shows no fracture but edema indicative of stress changes in the os naviculare.
Dr Blake's comment: The edema/swelling seen within the os navicularis/os tibial externum/accessory navicular can take months and months to resolve after the initial injury, so not an indication that things are not healing. The pain above the ankle was one of the tendons trying to help out the injury: FDL, PT, FHL, or AT. When one area is injured, the surrounding muscles/tendons help out and do some extra work. That can make them hurt also. A Rule of Three tends to occur until the body re-establishes equilibrium---original problem, compensatory problem #1, and compensatory problem #2. The true injury is at the bump with the accessory bone however.
Dr Blake's comment: The edema/swelling seen within the os navicularis/os tibial externum/accessory navicular can take months and months to resolve after the initial injury, so not an indication that things are not healing. The pain above the ankle was one of the tendons trying to help out the injury: FDL, PT, FHL, or AT. When one area is injured, the surrounding muscles/tendons help out and do some extra work. That can make them hurt also. A Rule of Three tends to occur until the body re-establishes equilibrium---original problem, compensatory problem #1, and compensatory problem #2. The true injury is at the bump with the accessory bone however.
Current treatment is 6 weeks non weight bearing air cast, then progression back to activity. She has so far missed 4 months of training. Everything we seem to read is confusing relating to surgery vs conservative treatment. For a high level athlete looking at missing another 3-4 months is devastating. We are wondering if surgery would be a better option as everything we seem to read indicates non surgical treatments are not effective.
Dr Blake's comment: I am sorry the literature is so poor on this subject. Yes, some patients need surgery. Doctors have a hard time deciding on surgery on someone that age, so feet get dragged.
Dr Blake's comment: I am sorry the literature is so poor on this subject. Yes, some patients need surgery. Doctors have a hard time deciding on surgery on someone that age, so feet get dragged.
It is an impossible decision for a parent to make, since surgeries can have problems, and the patient can be worse (less than 10%). When they are worse, there is usually an explanation, but a second surgery is often needed after months and months of unsuccessful rehabilitation. For a professional athlete, paid big bucks, they have surgeries for speed of rehabilitation. Every second they miss playing cost the team money. But, in the non professional, and at a young age, you want to be very very sure that surgery is needed. I have treated 100s with this condition with less than 1% having surgery (and perhaps another 9-10% just stopping their activities to avoid surgery). So, 90% get better without surgery and can continue with their sport of choice at a high level, will your daughter be one of those?
Our doctor indicates feels that the literature supports good outcomes with nonsurgical treatment and that is what she recommends. Any information you can share to help us would be great. We just want to make sure that whatever treatment she receives limits the time out of sport and reduces the chance of recurrence.
Dr Blake's comment: The approach to getting this better, and keeping it better, is a multi-discipline approach.

The podiatrist/therapist/orthotist must make great orthotic devices to stabilize the injured arch/accessory bone. The physical therapist/trainer must develop a strengthening program, pain free, that gets the posterior tibial tendon, and the surrounding muscles/tendons, and the quads/core strong as the other side. Your daughter should be icing twice daily and contrast bathing for the bone edema once daily to remove the inflammation. She should be on a stationary bike, etc, pain free, up to one hour per day to get the legs strong for her return to activity. She needs to learn the best way to tape the area which gives her the best pain relief, since taping in soccer games/practices is crucial and more protective than orthotics. She should be in the deepest soccer shoe she can find. It is when the orthotics, tape, strength, pain level are right, she can go back to activity. The coach is probably the most vital part to this team.

She/he must be protective of your daughter, be vigilant for signs of limping, know when to rest her, when to play her, perhaps change positions temporarily to help the demands on that ankle/foot. If the coach can not do this, all our best plans are destroyed, and it gives conservative management a bad name. Make sure diet is very healthy, including at least (2) 4 ounce servings of red meat weekly, if she is not a red meat eater.

And, as parents, you need to get rid of any timeline right now as you read this. Honor her body tissue. Do not think about timelines, you will only get frustrated. Thank you so much.
So, in summary, here is your next 3 month assignment: Wean from Non weight bearing to weight bearing without increased pain.
- Perfect the orthotics
- Perfect the soccer cleats
- Avoid barefoot at home if that bothers the area
- Learn a variety of taping methods
- Ice and Contrast Bath daily
- Eat healthy
- Talk to the coach about a gradual return to soccer, and any ideas on position change
- Tell the physical therapist you want to learn a pain free gradual and progressive strengthening program so 6 months from now you/she have tendons of steel (at least 3 times stronger). Good Luck!!

And the response:
Dr. Blake,
Thank you so much for your information. As a result of the info you provided we decided to seek a second opinion from an orthopedic surgeon. His diagnosis correlated with your info. He recommended casting in a walking boot for the next 3 weeks but did not feel NWB was necessary or appropriate. This is great news for us as this is not a stress fracture of the navicular as we were being told was a possibility as well . She is allowed to walk in the boot and swim which will decrease unnecessary deconditioning and ankle stiffness. He also said surgery may be an option using a modified kidner only if conservative measures fail. He recommended physical therapy and orthotics. Thank you again. It is nice to finally have a clear diagnosis and logical treatment options backed by two professionals.
Accessory Navicular: An Accessory You May Want To Do Without
This email was received from a patient suffering from a syndrome of pain produced by a weakened attachment of the posterior tibial tendon into the navicular. The posterior tibial tendon is the strongest supporter of the arch. The weakened attachment is due to an extra bone next to the navicular at the height of the arch. This extra bone occurs in probably 3% of the population and is called accessory navicular, os navicularis, os tibial externum, and the extra ankle bone. In only 10% of those patients with it does it occur on the other side also (bilateral).
Hello Dr. Blake,
I am a 29 year old who has been suffering from a lot of foot pain since early childhood-- it wasn't until I was in highschool that the Dr. examined me standing and realized that my arches "collapse". Finally they took an x-ray and found that I have bilateral accessory naviculars. I have since worn orthotics and attempt to wear very stable shoes (i.e. Saucony Hurricane). Due to the pain, I cannot do high impact sports, and walking long distances usually results in pain and limping. (I will also get shooting pain up my shins, in my knees, or in my thighs/hips). There are not too many shoes I can wear comfortably, and even with my orthotics I will have pain if I walk
more than a mile or so.
 |
X ray shows accessory navicular under the navicular at the height of the arch.
|
Dr Blake's Note: The os tibial externum begins to form around 8-9 years old, and should be fully formed at 16 years old. It can fully attach bone wise, or partially attach with cartilage or fibrous tissue. These last 2 attachments are particularly weak and can cause pain.
 |
This MRI view of an Accessory Navicular shows it inferior and closer to the heel than the big toe.
|
In the past, my foot doctor has suggested that if pain cannot be improved with orthotics, I should consider having them surgically removed. The Dr. mentioned that most people have pain from the bones rubbing on shoes, etc, which I have never found rubbing to be a problem, more like pain from misalignment. I did PT for a while, and much of the focus was on stretching and strengthening muscles, especially my hips. While this did help with aches in knees/hips/thighs at the time, I don't really feel like my overall strength or balance has improved.
Dr Blake's Note: I have never had a patient with this syndrome with pain limited to shoe rubbing, since orthotic devices, shoe padding, and taping all take the pressure off the outside of the bone. The real pain is from something else, and that is what needs to be discovered . Discovering where the pain is coming from hopefully will enable the patient to avoid surgery, since the treatment can be directed at that, or if surgery is necessary, make sure the right surgery is performed.
I also have very poor balance, tight achilles tendons and hamstrings,
and weak muscles.
Dr Blake's Note: If you read the discussions later on posterior tibial and arch strengthening, you will understand the complexity to strengthening through pain. If the tendon is damaged, you will not be able to strengthen it, and surgery may be necessary. If the tendon is not damaged, it is vitally important to attempt to isolate it and strengthen it, pain-free, and not strengthen the peroneals at all.
I also apparently have possibly pinched nerves between my big toe/second/possibly third toe at times when walking-- the area above and between by big and second toe will swell a bit and I get tingling/pain//numbness in my third toe sometimes when walking.
Dr Blake's Note: The significance of this statement is that Lindsey may have a version of Tarsal Tunnel syndrome which gives posterior tibial symptoms, and also superficial toe nerve symptoms. This would be a rare situation, so I will ignore it right now, but keep the info somewhere in the recesses of the brain.
Recently, I made the silly mistake of wearing sandals to the mall. After walking around, my right foot began hurting, and has been getting worse (now on day two). The pain is located directly below my ankle on the inside in a very localized spot, and has been swollen. I have been icing it and it helped minimally (I also tried tylenol). It hurts regardless of movement, bearing weight, etc.
Dr Blake's note: also perhaps Tarsal Tunnel??
Dr Blake's note: Like many of these chronic problems, they can become acute at times. The mistake made now is not to recognize that you have to treat this acute injury first, and deal with the chronic injury after. Lindsey is now in the Acute Phase of Rehabilitation (for this chronic injury). The treatment is immobilization and anti-inflammatory. Get yourself into a removable Anklizer Boot and ice 3 to 4 times a day for 15 minutes. If the ice irritates the local nerves, ice 3 inches above the area, and consider a Rx of voltaren gel 4 times daily or Flector Patches every 12 hours. Should be better in 1 to 2 weeks.
I tend to "hold my arches up" and transfer more weight to the outside edges of my feet, because letting my arches collapse immediately causes pain and irritation.
Dr Blake's Note: This is what the orthotic devices must do for a patient. They must be designed to hold up the arch, perhaps along with Kinesiotape, so that the patient doesn't strain the tissue further doing it using muscles and tendons abnormally.
I was told by my Dr. that the tendon holding my arch up is partially connected to the accessory navicular, making my arch unstable and collapse. ( I have also been told in the past that I have "loose ligaments-- but I have noticed that while I am very flexible in some joints, I am extremely tight elsewhere).
Dr Blake's Note: If you imagine that only 1/2 of your achilles tendon attached where it should, and the other 1/2 attached into a soft ligament, you would not have only 1/2 the strength, you would have next to nothing. As the achilles pulls, the weakest link in the chain (the part not attaching into solid bone) would begin to strain, and the whole achilles begin to hurt. Same with the accessory navicular, the part of the posterior tibial tendon that does not attach into solid navicular begins to strain trying to stabilize the foot, and slow down pronation of the foot, ankle, knee, sooooo pain ensues. It can not do it's job properly.
I am not sure what sort of direction is best with this problem. I don't know if this swelling/pain is from the extra bones and would diminish with surgery, or not. The pain is so frustrating and keeps me from being active too much at all-- I enjoy dance, walking, yoga, cycling and swimming-- but often walking and dance are limited (and running is out of the question) due to the pain it will cause.
Dr Blake's Note: Once the acute pain is gone, and you are back to dealing with only chronic pain, you need to get this worked up. I will give my final recommendations below, but you must know my recommendations center around a world that I would like, maybe not practical.
It seems like my pain is not the usual for accessory navicular (as according to Dr.) so I am not sure if this is an unusual case? Any advice or information on this would be great. This has been causing trouble for most of my life (i.e. being unable to enjoy walks/hikes/sports, having trouble falling asleep due to pain, pain and limping at work).
Thanks,
Lindsey
Lindsey
 |
MRI view on the partial bone attachment of the accessory navicular.
|
Dr Blake’s response:
Lindsey, Most of the pain from this syndrome can be from inflammation at the attachment of the posterior tibial into the accessory navicular, actual tearing of the tendon itself, injury to the spring ligament just under this bone, chronic movement of the accessory bone on the parent bone (navicular) like in a fracture non-union, or originating from another structure (both tarsal coalition and tarsal tunnel syndromes can have similar presentations at times). Please read the section entitled Tip of the Iceberg since sometimes the apparent problem is actually not what is producing pain. You are definitely a surgical candidate due to the length of time you have had this. That being said you need a good work up to make sure they operate on the right area and do the right thing for you. And, you may find along the way that you don't need surgery. So, if I could prioritize wish lists for you, they would like this:
- Get the acute pain calmed down with an Anklizer Boot, an EvenUp for the other side, anti-inflammatory. You will need the boot and EvenUp again.

- Get an MRI to look at the tendon, attachment of the bones, spring ligament, tarsal coalition, and tarsal tunnel areas.
- If the MRI shows a lot of bone activity, get a bone scan.
- Talk to a Physical Therapist about isolating the posterior tibial tendon during strengthening. Can you do at least isometrics without pain? Begin strengthening the tendon, same exercises are needed post operatively. Strengthening should only be done in the hour before bed, and ice after even if it does not hurt.
- Get an orthotic that is comfortable, but supports your arch. Are there doctors or therapists in your area that use a version of the Inverted Orthotic Technique? You must feel that the orthotic works so well that you do not need to pull up your arch.
- Ice three times daily period. For 15 minutes each. Since you can wrap ice around the top and inside of your foot and walk around the house, at least you can do other things.
- Learn to Kinesiotape your arch or check out the tape from suportthefoot.com. Tape daily. You can ice through it.
- Do not go around with sandals or barefoot. Dansko clogs may work. A compromise may be an Orthaheel or Chaco Sandal with Kinesiotape.
- Feel free to send me any tests along the way. You have a big journey. Hang in there. Be Logical. I hope this has helped. Rich
I strained my accessory naviular syndosmosis 8 months ago. MRI showed no PTT tears and very minimal bone oedema. I am in orthotics and some days are pain free but some days I get an ache around the area or more proximally up the PTT, pain 1-2/10 max. I can cross train, row and cycle but am doing no impact activity. My orthopaedic surgeon told me that if it was going to settle it would have done by now and that the next step to consider is surgery (he recommended a Kinder procedure). Given how much better it has got and fairly positive MRI results I would like to think that conservative treatment could work for me but lack guidance as to how to go about it. Should I be considering surgery at this point? Can delaying surgery affect how successful the outcome is? Many thanks in advance.
ReplyDeleteAlexandra, doing surgery now is like recommending preventative surgery. I have not heard you talk about strengthening exercises. You need to gradually, and pain free, strengthen the PT tendon, and other tendons/muscles that support your arch. You need to maximize the amount of arch support you get from your othotic devices. You need to do posterior tibial taping for all your athletic activities. Hope this helps. Rich
DeleteI never believed i would be healed from HIV someday. And I have been taking some medication from my doctor and there was no improvement. Few weeks ago i came on search on the internet if i could get any information concerning the prevention of this disease, on my search i saw a testimony of someone who has been healed from (HSV 2 and Cancer) by this Man Dr Sayo and she also gave the contact of this man and advise we should contact him for
Deleteany sickness that he would be of help, so i wrote to Dr Sayo telling him about my (Hiv virus ) he told me not to worry that i was going to be cured!! hmm i never believed it, well after all the procedures and remedy given to me by this man
few weeks later i started experiencing changes all over me as Dr, Sayo assured me that i have cured,after some time i went to my Doctor to confirmed if i have be finally healed, behold! it was TRUE, So friends my advise is if you have such sickness or any other at all
you can reach Dr Sayo on his email, (sayoherbalhealer@gmail com) .....ALL THANKS TO GOD FB page https://www.facebook.com/Sayo-Herbal-Healer-100145798345000/ check blog: https://sayoherbalhealer.blogspot.com/
I never believed i would be healed from HIV someday. And I have been taking some medication from my doctor and there was no improvement. Few weeks ago i came on search on the internet if i could get any information concerning the prevention of this disease, on my search i saw a testimony of someone who has been healed from (HSV 2 and Cancer) by this Man Dr Sayo and she also gave the contact of this man and advise we should contact him for
any sickness that he would be of help, so i wrote to Dr Sayo telling him about my (Hiv virus ) he told me not to worry that i was going to be cured!! hmm i never believed it, well after all the procedures and remedy given to me by this man
few weeks later i started experiencing changes all over me as Dr, Sayo assured me that i have cured,after some time i went to my Doctor to confirmed if i have be finally healed, behold! it was TRUE, So friends my advise is if you have such sickness or any other at all
you can reach Dr Sayo on his email, (sayoherbalhealer@gmail com) .....ALL THANKS TO GOD FB page https://www.facebook.com/Sayo-Herbal-Healer-100145798345000/ check blog: https://sayoherbalhealer.blogspot.com/
Acupuncture treatments have documented to be great success in treating injuries related to tense, scarred or irritated tendons, nervous tension or muscles. Mississauga acupuncture is also a good treatment for depression and some allergies.
ReplyDeleteI was diagnosed with accessory naviculars a few years ago, and custom orthotics and good tennis shoes have greatly reduced my pain for day-to-day activities.
ReplyDeleteI did, however, enjoy hiking, but now my feet (in tennis shoes with orthotics) hurt on relatively short hikes, especially going down hill. Do I have any hope of hiking pain-free again? Any magical hiking boots?
Thank you!
Sometimes hiking needs the Aircast Airlift PTTD Brace or strong posterior tibial taping that is describing in the blog. Use the Leukotape version. You can also increase the support from the orthotics. Ask the doctor to up the correction 10% on another pair to see if you can tolerate. Typically they have to raise the medial arch and also the lateral heel cup to make sure you do not go to far out. Hope this helps. Rich
DeleteDr Blake, My daughter is 9 years old and started having feet pain off and on last summer. Since January it became more consistent and now it is daily. We initially went to a orthopedic doctor and he referred to PT and a podiatrist. In the mean time we bought New Balance shoes and insoles. She btw was determined to have collapsing arches that had apparently aggravated the supporting tendon. During PT we started noticing a place on the inside of her left foot that now protrudes all the time and is very tender. We have also been to our family physician. Everyone just wants her in arch supporting insoles. We have been given anti inflammatory creams as well. Nothing works! We have tried all creams, advil, several different insoles, icing, stretching and physical therapy. We also took her out of karate, and reduced other activities. My daughter is in pain every day. They say her xrays are normal. Below the navicular bone there are 3 little pebble looking shapes. I am wondering if that extra bone is forming??? I am just at a loss of what to do next. Every shoe we have seems to really aggravate the protrusion on the inside of her foot. Any advice would be appreciated.
ReplyDeleteJennifer, thank you for your comment. Definitely sounds like the beginning of accessory navicular syndrome for sure. Buy some 1/4 inch adhessive felt which you can adjust/thin as needed to build a horseshoe accommodation for shoes. You really need to get her into a removable boot for 3 months to begin the Immobilization Phase ASAP. This should be accompanied with 10 minute ice packs three times a day. Since there is always time a home that she will walk without the boot, she will know if it is getting better. You stay completely in the boot 2 weeks longer than you need to. During the boot time, you have a podiatrist make a custom orthotic device with an accommodation. Hope this helps your daughter heal faster. Rich
DeleteGood article. Keep sharing such a useful post.
ReplyDeleteAcupuncture Specialists in Chennai
Dr. Blake I am extremely excited to find your blog. Last year I had a Modified Kidner Procedure on my right foot. I had a large accessory navicular bone that was rubbing against the navicular bone. According to my surgeon the damage to the PTT was minimal, but the cartilage between the bones had worn away, and it was bone rubbing against bone. It's been 13 months since my surgery, and I have resumed many of my normal activities at a more conservative level. Prior to the surgery I was a marathoner, now I'm content with shorter distances at a slower pace. Recently I've developed some cramping in my surgery foot. It feels like a charley horse in the arch of my foot, but in the tendon instead of the muscle. The only change I can identify is that my dressage trainer had me shorten my stirrups during my riding lesson which increased the degree of plantar flexion in that foot. That night I experienced the first cramp. I immediately lengthened my stirrups the next day, but my foot keeps cramping. Do you have any suggestions as to what might be going on? I've been working on slowly increasing strength and flexibility in the foot over the last year. Could I have overdone it during my riding lesson? I would really like to avoid a second surgery. Any suggestions would be greatly appreciated.
ReplyDeleteThank you!
Krissy
Dr. Blake,
ReplyDeleteI am very happy to find your blog. Make my story short. I have flat foot, accessory navicular syndrome(which I don't know until now).
52 years old female. June, 2016, do calf-raise, stand up like ballet dancer. (my tendon is pretty weak). Right after that, feel like sprain ankle, but no swollen from outside. Just hurt inside ankle bone area. See orthopedic and he send me to physical therapy for 6 weeks. Recovered a lot, after 2 month, re-injury just do calf-raise and elliptical machine. Now, I done MRI(last week). Result is:
Type 2 accessory navicular with mild degenerative change in subcortical edema across the synchondrosis. Posterior tibial tendon(and other) all normal. Question is, orthopedic surgeon suggest surgery remove that extra bone. Wonder will the edema heal without surgery ?
Thanks
Dominica L.
This comment has been removed by the author.
ReplyDeleteDr. Blake,
ReplyDeleteI was very happy to find you blog, it's very detailed and the way you explain things is very easy to understand. 2 years ago I had a bad fall/sprain. X-ray didn't show anything so for 6 months I was limping around with a swollen and bruised foot. After a little over six months things somewhat improved, I still had some swelling but I was able to walk without limping with some discomfort (going down the stairs, walking/standing extended periods of time etc..). It has now been almost two years, I still experience discomfort when going down the stairs and walking/standing a lot. They repeated an x-ray and did an MRI which showed a chronic appearing ossicle at the medial navicular with pseudoarticulation, edema and sclerosis on both sides. The orthopedic surgeon I consulted with, recommended surgery (Kidner procedure) but since I had not tried any conservative measures, I asked to do that first. I only went to therapy twice due to a high deductible, got some exercises to do at home, I also have an ankle brace, which really helped while on but increased my pain once I took it off. One day after wearing the brace all day, my pain was so excruciating and my foot so swollen that I started limping again. A huge set back. My pain was never gone, but at least before I was able to walk around without limping with only some discomfort based on what I was doing. I was contemplating based on your previous suggestion to other patients, getting an ankle stabilizer/boot. I'm just afraid that after immobilizing my foot for 3-4 weeks, once I take it off I will have even more issues... any suggestions to avoid surgery? I'm a mom of a 4 years old and a 7 month old and It's so hard to be off my feet and let this foot heal properly! Thank you in advance for all your help!
In response to your original post. Does anyone have any idea what brand and style of soccer cleats work best for over pronation and accessory navicular? We have custom orthotics for my daughter, but soccer cleats can often be tight and push on the accessory navicular, especially when she kicks.
ReplyDeleteGreat article. I learned lot of things. Thanks for sharing. I figure that they having a great time to peruse this post,they might take a decent site to make an information. free mri viewer
ReplyDeleteYou there, this is really good post here. Thanks for taking the time to post such valuable information. Quality content is what always gets the visitors coming. tratamiento de la agorafobia
ReplyDeleteThe foot and ankle surgeon will ask about symptoms and inspect the foot to look for skin irritation or edema before diagnosing accessory navicular syndrome. The physician could apply pressure to the bony protrusion to feel for any pain. The patient's gait pattern, foot anatomy, muscle strength, and joint mobility can all be assessed.
ReplyDeleteGood afternoon, I have AN in both ankles. Wore a boot for 6 weeks and then the first doctor changed his mind about wearing the boot for 6 weeks on the second foot and prescribed therapy. I went to get a second opinion and the second doctor advised against therapy and continuance of the boot and recommended steroids. What are your thoughts on steroids (pill form) for a week and vitamin D? Doctor recommended this, but I’m having a hard time finding research on it and debating if I should consider taking steroids/vitamin D as the doctor recommended or if I should start therapy. U really don’t like to have to take pills or surgery if I don’t have to and there are better alternatives. Doctor advised against physical therapy and boot. He wants to try this the steroids first..
ReplyDelete